Loading
Get Attending Physicians Return To Work Recommendations To Be Completed By Attending Physician Reviewed
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Attending Physicians Return To Work Recommendations To Be Completed By Attending Physician Reviewed online
This guide provides a clear and supportive overview of how to fill out the Attending Physicians Return To Work Recommendations form online. Follow the step-by-step instructions to ensure accurate completion for effective communication regarding the patient's ability to return to work.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to access the form and open it in the online editor.
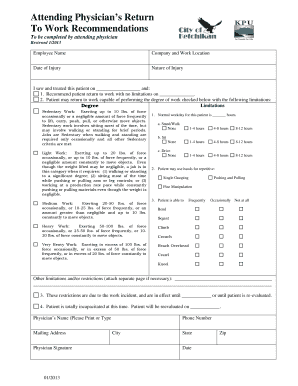
- Begin by entering the employee's name in the designated field. This identifies the individual for whom the recommendations are being made.
- Fill in the company name and work location. This information is crucial for contextualizing the patient's employment situation.
- Specify the date of injury. This will help track the timeline of the patient's recovery process.
- Describe the nature of the injury briefly. This helps in understanding the context of the patient's limitations.
- Document the date you saw and treated the patient, which is necessary for record-keeping and follow-up evaluations.
- Choose whether you recommend the patient return to work with no limitations or with specified limitations. If there are limitations, proceed to the next fields.
- Indicate the type of work the patient may return to and check the appropriate degree of work (sedentary, light, medium, heavy, or very heavy).
- Specify the normal workday activities for the patient, such as standing, walking, sitting, and driving, by marking the relevant hours they can perform these tasks.
- Indicate the patient's ability to perform repetitive tasks using their hands by marking the frequency of actions like single grasping, pushing, pulling, or fine manipulation.
- Document any additional limitations and/or restrictions. If necessary, attach a separate page for detailed descriptions.
- Clarify that the restrictions are due to the work incident and indicate when these restrictions will be effective until or when the patient will be reevaluated.
- If the patient is currently incapacitated, confirm this and specify when they will be reevaluated.
- Finally, provide the physician's name and mailing address. Sign the form and include the date, phone number, city, state, and zip code to ensure all contact information is accurate.
- Save the changes you've made, and consider downloading, printing, or sharing the completed form as necessary.
Complete your documents online today to facilitate smooth communication regarding return-to-work recommendations.
An Attending Physician Statement (APS) is a questionnaire form that the insurer asks your physician to complete in order to assess your health and determine your insurability.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.