Loading
Get Medicare Claims Processing Request Mcps Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medicare Claims Processing Request MCPS Form online
Filling out the Medicare Claims Processing Request MCPS Form online is a crucial step in ensuring your access to the Medicare Claims Processing System. This guide will provide you with clear, step-by-step instructions to navigate the form efficiently and successfully.
Follow the steps to complete your form with ease:
- Click ‘Get Form’ button to obtain the form and open it in the editor.
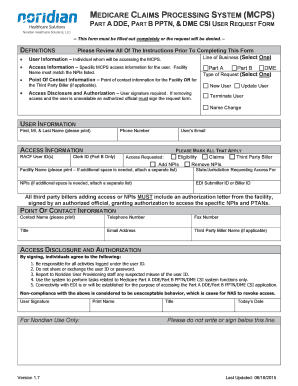
- Indicate the line of business for which you are requesting access by marking one of the following options: Part A for facility services, Part B for physician services, or DME for supplier.
- Provide your user information, including the first name, middle initial, and last name of the user requesting access, as well as their direct phone number and email address.
- In the access information section, include the existing RACF User ID if you are an existing user. If you are a new user, leave this blank unless you have an existing User ID with another contractor.
- Specify the access you are requesting. This may include marking options such as eligibility, claims, or any third-party billing information.
- Provide the name of the facility linked to the user's access, ensuring it matches the NPI listed. If multiple facilities are involved, note that in an attached list.
- List all states or jurisdictions where access is being requested. If applicable, indicate the specific jurisdiction for DME.
- For third-party billers, an authorization letter from the facility is required, attaching it to the request form to validate access to the NPIs.
- Complete the point of contact information by specifying a contact person's details, including their phone number, fax number, title, and email address.
- In the access disclosure and authorization section, ensure the user signs and dates the form. If the user is unavailable, an authorized official must provide their signature.
- Once the form is filled out completely, fax the completed form to the designated number. Remember that email submissions will be rejected.
Start completing your Medicare Claims Processing Request MCPS Form online today for timely access.
Related links form
Contact Contact. 855-609-9960.