Loading
Get Provider Subcontractor Disclosure Of Ownership Controlling Interest Worksheet
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Provider Subcontractor Disclosure Of Ownership Controlling Interest Worksheet online
Filling out the Provider Subcontractor Disclosure of Ownership and Controlling Interest Worksheet is a crucial step for health plans and providers to ensure compliance with federal regulations. This guide will walk you through each section of the form, making the process straightforward and accessible.
Follow the steps to complete your form accurately.
- Press the ‘Get Form’ button to access the worksheet. This will allow you to open the form in your preferred online editor.
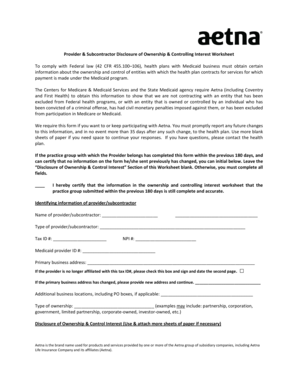
- Begin by entering identifying information for the provider or subcontractor. Fill in the name, type, Tax ID number, NPI number, and Medicaid provider ID. Ensure this information is accurate, as it is crucial for identification.
- Provide the primary business address of the provider or subcontractor. If the address has changed, indicate this and enter the new address. If there are additional business locations, list them as required.
- Specify the type of ownership. This could be a partnership, corporation, government entity, or another recognized business structure. Carefully select the appropriate type.
- In the Disclosure of Ownership & Control Interest section, begin by listing any individuals or organizations with a direct or indirect ownership of 5 percent or more in your entity. Include relevant details such as addresses and identification numbers as necessary.
- For each person listed in the previous step, clarify their relationship to other individuals with ownership. This helps establish connections that may exist in ownership interests.
- Continue by documenting any other entities where these individuals have an ownership or control interest, which is necessary for transparency.
- List managing employees' information, including their addresses, dates of birth, and Social Security numbers. This section identifies those in operational control and management of your entity.
- Check if any changes in ownership or control have occurred in the past year and provide the relevant dates. This is important for compliance with ongoing reporting requirements.
- Indicate whether any individual listed has been excluded from federal health programs or had civil penalties imposed. Provide details, if applicable, to ensure full disclosure.
- Finally, verify the completeness and accuracy of the information provided. Sign and date the form, affirming the truthfulness of your disclosures.
- Once you have filled out all necessary sections, save your changes. You may also download, print, or share the completed form as required.
Complete your Provider Subcontractor Disclosure Of Ownership Controlling Interest Worksheet online today to ensure compliance and facilitate your engagement with health plans.
Answer. Your name will appear on your diploma exactly how you specify on your graduation application. If you have a preferred first name that is not your legal first name, please be sure to put your preferred first name on your graduation application.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.