Loading
Get Nys Medicaid Prior Authorization Request Form For
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NYS Medicaid Prior Authorization Request Form online
This guide provides clear and comprehensive instructions on completing the NYS Medicaid Prior Authorization Request Form online. Following the outlined steps will ensure that all necessary information is submitted accurately to facilitate the authorization process.
Follow the steps to successfully complete the form.
- Click ‘Get Form’ button to obtain the NYS Medicaid Prior Authorization Request Form and open it in your preferred editor.
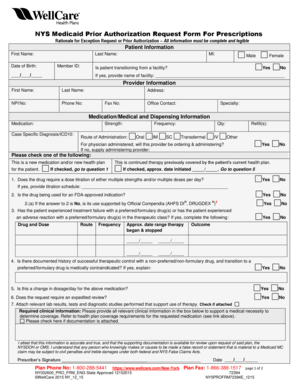
- Begin by filling out the patient information section. Enter the first name, last name, member ID, and middle initial. Indicate the patient's date of birth and gender, and if applicable, denote if the patient is transitioning from a facility by providing the facility's name.
- In the provider information section, complete the prescriber’s first name, last name, NPI number, telephone number, address, and fax number. Additionally, include a contact person's name and the provider’s specialty.
- Fill in the medication and medical dispensing information. Specify the medication's name, strength, case-specific diagnosis (ICD10), frequency, and route of administration. Indicate the quantity and any refills needed.
- Answer the questions related to prior medications. Indicate whether the drug requires a dose titration, if the drug is used for an FDA-approved indication, and if there has been treatment failure with a preferred/formulary drug.
- Attach relevant clinical information, supporting documentation, and laboratory results in the appropriate section of the form. Confirm that you have attached the necessary documents.
- Sign and date the form to attest that the information provided is accurate. Ensure that you include your contact information and that of the plan if applicable.
- Once the form is completed, you can save any changes made to it. Choose an option to download a copy of the form, print it for physical submission, or share it as needed.
Complete the NYS Medicaid Prior Authorization Request Form online today to ensure your prescription is authorized promptly.
Prior authorization (prior auth, or PA) is a management process used by insurance companies to determine if a prescribed product or service will be covered. This means if the product or service will be paid for in full or in part.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.