Loading
Get Medicare Redetermination Request Form 1st Level Of Appeal - Cms
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Medicare Redetermination Request Form 1st Level of Appeal - Cms online
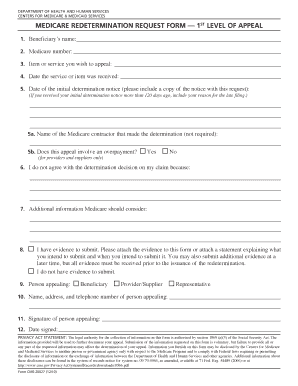
The Medicare Redetermination Request Form allows users to appeal a decision made by Medicare regarding coverage or payment for a specific item or service. Filling out this form correctly is crucial for ensuring that your appeal is considered in a timely manner.
Follow the steps to successfully complete the form.
- Press the ‘Get Form’ button to access the form and open it in your document editor.
- Provide the beneficiary’s name in the first field. This should be the name of the individual who received the Medicare benefits.
- Enter the Medicare number in the second field. This number is important to identify the beneficiary’s account.
- In the third field, specify the item or service you wish to appeal. Be as detailed as possible to avoid confusion.
- Provide the date the service or item was received in the appropriate field. This helps establish the timeline of your appeal.
- In the sixth field, indicate the date of the initial determination notice. Remember to include a copy of this notice with your request.
- If applicable, mention the name of the Medicare contractor that made the determination in the next field; although this is not required.
- For the eighth step, indicate whether this appeal involves an overpayment by selecting Yes or No. This is relevant for providers and suppliers only.
- Detail your disagreement with the determination in the next section, explaining clearly why you believe the decision should be reversed.
- In the subsequent field, provide any additional information that Medicare should consider regarding your appeal.
- If you have evidence to submit, mention it here. You may attach the evidence now or provide a statement about when you will submit it.
- Indicate the role of the person appealing by selecting Beneficiary, Provider/Supplier, or Representative in the designated section.
- Fill in the name, address, and telephone number of the person appealing in the next fields.
- Have the person appealing sign the form in the signature field.
- Finally, enter the date the form is signed. Ensure all information is accurate before saving, downloading, printing, or sharing the completed form.
Start your appeals process today by completing the Medicare Redetermination Request Form online.
Faxing Your Redetermination Request — You can fax the redetermination request to us along with the documentation that is needed to determine if the services are medically necessary and covered under Medicare's guidelines.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.