Loading
Get Authorization For Release Of Medical Information - Uwhealth
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Authorization For Release Of Medical Information - Uwhealth online
Filling out the Authorization For Release Of Medical Information form for Uwhealth is a straightforward process. This guide provides step-by-step instructions to help you complete the form accurately and efficiently, ensuring your medical information is released according to your preferences.
Follow the steps to complete the form effectively.
- Press the ‘Get Form’ button to access the Authorization For Release Of Medical Information form and open it in your online editor.
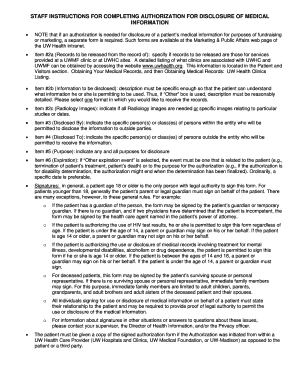
- In the patient information section, fill in your name (last, first, middle initial), street address, city, state, zip code, date of birth, and phone number. Ensure that all details are accurate.
- For item 2a, indicate where the records will be released from by checking the appropriate box: UW Hospital and Clinics, UW Medical Foundation Clinics, both, or UW Rehabilitation Hospital.
- In item 2b, specify what medical records you wish to disclose. Choose between a comprehensive overview of your chart, records pertaining to specific conditions, or a complete copy of your official medical record. Select one format for receiving the records: paper or DVD.
- In item 2c, denote whether you require all radiology images or specify which images are needed based on dates or studies.
- For item 3, indicate who within your healthcare provider's organization is authorized to disclose your medical information.
- In item 4, specify the persons or entities outside the organization that you authorize to receive your medical information.
- Outline the purpose of the disclosure in item 5 by checking all applicable reasons for your request.
- In item 6, determine the expiration of the authorization. If you choose 'Other expiration event,' provide a relevant event or date.
- Finally, sign and date the form. If someone else is signing on your behalf, specify their relationship and authority to do so.
- After completing the form, review it for accuracy. Users can then save any changes made, download a copy, print it out, or share the form as needed.
Complete your Authorization For Release Of Medical Information online today to manage your medical records effectively.
Related links form
The Health Insurance Portability and Accountability Act of 1996 was put in place to help ensure the privacy and ease of access of your medical records. A HIPAA authorization form is a document in that allows an appointed person or party to share specific health information with another person or group.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.