Loading
Get Nova Healthcare Prior Authorization Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Nova Healthcare Prior Authorization Form online
Filling out the Nova Healthcare Prior Authorization Form online is a straightforward process that ensures your medical needs are communicated effectively. This guide will provide step-by-step instructions to help you complete the form accurately and efficiently.
Follow the steps to complete the form successfully.
- Click ‘Get Form’ button to access the Nova Healthcare Prior Authorization Form and open it in your preferred browser.
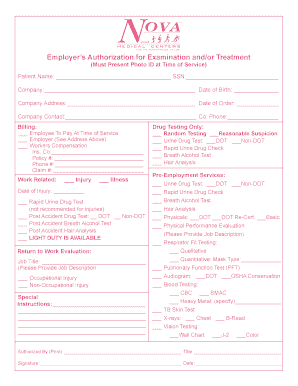
- Begin by entering the patient's name in the designated space at the top of the form, followed by their social security number. Ensure that the information is accurate to avoid delays.
- Provide the company name and complete the date of birth field for the patient. This information helps verify the identity of the patient and their association with the employer.
- Fill in the company address and the date of order, which are essential for processing the authorization request. Confirm that the details match the company's records.
- List the company contact person’s name and phone number for any follow-up communications. This step is crucial for clarifying information if needed.
- Select the billing option that applies: whether the employee will pay at the time of service, the employer will cover the costs, or if it's a worker’s compensation case.
- Input the insurance company details, including the policy number, phone number, and claim number if applicable. These specifics facilitate claims processing.
- Indicate whether the case is related to a work-related injury or illness by checking the appropriate box. Include the date of the injury if applicable.
- Fill out the drug testing section if required, specifying the type of tests ordered, such as urine drug tests, breath alcohol tests, or hair analysis.
- Complete the return-to-work evaluation section by providing the job title and brief job description. Indicate any special instructions necessary for the evaluation.
- Sign and print your name in the authorized by section, including your title and the date of submission. This signature verifies your approval of the information presented.
- Once all fields are complete, review your entries for accuracy. After verifying the information, you may save changes, download, or print the completed form for submission.
Complete your forms online today for a more efficient processing experience.
Nova Healthcare Administrators, an Independent Health company, is the administrator of your Reimbursement Account(s) which may include Flexible Spending Accounts (FSA), Health Reimbursement Arrangements (HRA) and Qualified Transportation Accounts (QTA).
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.