Loading
Get Almadallah Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Almadallah Claim Form online
Filling out the Almadallah Claim Form online is a straightforward process that ensures your reimbursement is processed efficiently. In this guide, we will take you through each section of the form, providing detailed instructions tailored to your needs.
Follow the steps to complete your Almadallah Claim Form accurately.
- Click ‘Get Form’ button to access the Almadallah Claim Form and open it in your chosen editor.
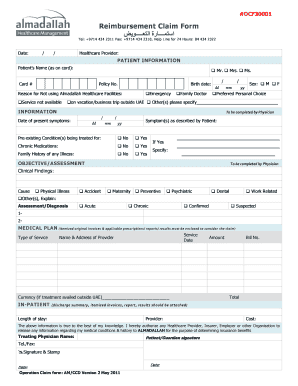
- Begin filling in the date at the top of the form. Be sure to format it as day/month/year.
- In the patient information section, enter the patient’s name as it appears on their card. Select the appropriate title: Mr., Mrs., or Ms.
- Input the patient's birth date in the specified format.
- Section for physician input: Enter the date of present symptoms and the symptoms described by the patient.
- Document any family history of illness by checking yes or no and providing specified details if applicable.
- In the medical plan section, ensure to list itemized original invoices along with applicable prescriptions and reports.
- For in-patient claims, fill in the length of stay, provider details, and total costs.
- Review the completed form for accuracy. Save any changes, and then download, print, or share the finalized version of the form.
Complete your Almadallah Claim Form online today to ensure a smooth reimbursement process.
For example, if you visit an out-of-network doctor, your insurer may agree to pay 130 percent of the rate Medicare would normally pay for the visit. This means that if Medicare would normally pay $100 for an office visit, your insurer would agree to pay up to $130.