Loading
Get Prior Authorization Worksheetperscription Order Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Prior Authorization Worksheetperscription Order Form online
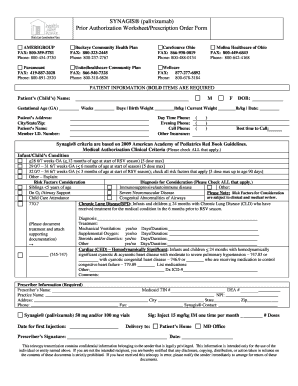
Filling out the Prior Authorization Worksheetprescription Order Form online is an essential step in ensuring the necessary approvals for treatment with ® (). This guide will walk you through each section of the form, providing detailed instructions to help you complete it accurately and efficiently.
Follow the steps to successfully fill out the form.
- Click ‘Get Form’ button to access the form and open it in your online editor.
- Enter the patient’s information in the designated fields, making sure to fill in the name, date of birth, gestational age, birth weight, and current weight. Note that fields marked in bold are required.
- Provide the patient’s address, including city, state, and zip code. It is also important to fill in the member I.D. number and contact numbers for day time, evening, and cell phone.
- Indicate if the patient has other insurance and specify the best time to contact.
- Check all applicable medical authorization clinical criteria based on the patient’s condition and gestational age as outlined in the AAP guidelines.
- Fill in the diagnosis section by checking all risk factors that apply to the patient, providing any other relevant diagnosis information.
- Document any treatment the patient has received, including duration and type, particularly for chronic lung disease if applicable.
- Complete the prescriber information section by entering the prescriber’s name, TIN number, DEA number, practice name, and contact details.
- Indicate the date for the first injection and specify the sig and number of doses required.
- Review all entered information for accuracy. After confirming the details, you can save changes, download, print, or share the form as needed.
Begin filling out your Prior Authorization Worksheetprescription Order Form online today to ensure timely processing and approval.
A CVS/Caremark prior authorization form is to be used by a medical office when requesting coverage for a CVS/Caremark plan member's prescription. A physician will need to fill in the form with the patient's medical information and submit it to CVS/Caremark for assessment.