Loading
Get Mercy Care
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Mercy Care online
Filling out the Mercy Care dental prior authorization request form online is a straightforward process that ensures your dental treatment is properly authorized. This guide will walk you through each section of the form, helping you provide the necessary information accurately and efficiently.
Follow the steps to complete your Mercy Care dental request form
- Click ‘Get Form’ button to acquire the form and open it in the editor.
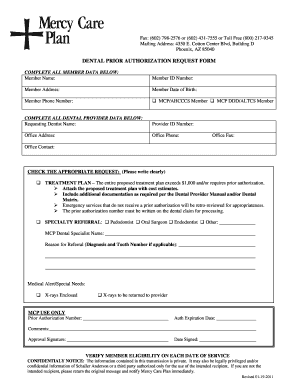
- Complete all member data by entering the member's name, ID number, address, date of birth, and phone number. Be sure to choose whether the member is a MCP/AHCCCS member or a MCP DDD/ALTCS member.
- Fill in all dental provider data, including the requesting dentist's name, provider ID number, office address, phone number, fax number, and contact name.
- Indicate the appropriate request by checking the applicable box. If selecting 'Treatment Plan,' ensure to attach the proposed treatment plan along with cost estimates and any additional documentation as required. Note that emergency services without prior authorization will be retro-reviewed.
- If applicable, select the specialty referral by checking any of the specialty types such as pedodontist or oral surgeon and provide the name of the MCP dental specialist and the reason for the referral, including the diagnosis and tooth number if needed.
- Include any medical alert or special needs information in the designated area and indicate whether X-rays are enclosed or to be returned to the provider.
- Once all fields are completed, ensure you save your changes. You can then download, print, or share the form as necessary for your records or submission.
Complete your Mercy Care dental prior authorization request form online today to ensure a smooth processing of your dental treatment.
Related links form
Mercy Care is a not-for-profit health plan serving AHCCCS members throughout Arizona. Owned by Dignity Health and Ascension Health, Mercy Care has served Medicaid members since 1985.