Loading
Get Provider Review Form - Bcbsmt
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the PROVIDER REVIEW FORM - Bcbsmt online
Completing the PROVIDER REVIEW FORM - Bcbsmt online is a straightforward process that helps ensure timely reviews of claims. This guide will walk you through each section of the form, offering step-by-step instructions to assist you in providing all necessary information accurately.
Follow the steps to effectively complete the provider review form
- Click the ‘Get Form’ button to access the provider review form and open it in your preferred editor.
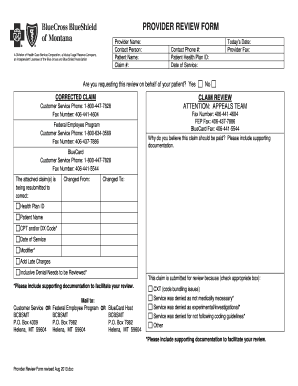
- Begin by entering the provider name and contact person in the designated fields. Ensure that these details reflect the correct information as it will help in identifying the reviewer.
- Fill in the patient name and claim number. These are essential for linking the review to the specific patient and claim.
- Provide contact phone number and patient health plan ID. This information is crucial for communication regarding the claim review.
- Indicate the date of service accurately. This ensures that the review is related to the correct service date.
- Specify whether you are requesting the review on behalf of your patient by selecting 'Yes' or 'No'. This conveys the context of your request.
- If applicable, indicate if this is a corrected claim by providing the necessary details in the corresponding fields. Be clear on what changes are being made.
- State the reasons why you believe the claim should be paid. It is important to include any supporting documentation that bolsters your request.
- Check the appropriate box indicating the reason for the review, such as coding issues or denial of medical necessity. Include relevant details and documentation.
- Review all entered information for accuracy to ensure the claims process proceeds without delay.
- Once all information is complete, save your changes, and consider downloading or printing a copy for your records or to share as required.
Complete and submit your provider review form online to ensure your claims are reviewed efficiently.
Call us at 1-866-940-3022 (TTY 711). We're open between 8 a.m. – 8 p.m., local time, 7 days a week.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.