Loading
Get Mail Completed Form To Healthscope Benefits P O Box 3594 Little Rock Ar 72203 3594
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Mail Completed Form To Healthscope Benefits P O Box 3594 Little Rock Ar 72203 3594 online
Filling out the Mail Completed Form to Healthscope Benefits is an essential process for ensuring that your claims are processed without delay. This guide will provide clear and supportive instructions on completing this form online, so you can submit your information accurately and efficiently.
Follow the steps to successfully complete your form.
- Click the ‘Get Form’ button to access the form and open it in your browser.
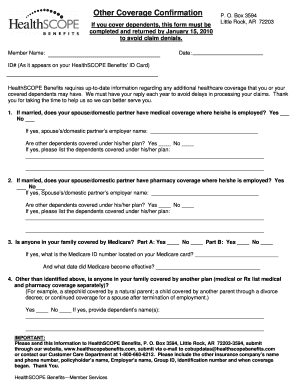
- Enter your full name in the 'Member Name' field. Ensure that this matches the name associated with your Healthscope Benefits ID.
- Provide the current date in the designated area; this helps to keep track of submission timelines.
- In the 'ID#' field, enter your Healthscope Benefits ID number as it appears on your ID card to assist in identifying your account.
- If you are married or have a domestic partner, indicate whether they have medical coverage where they are employed by selecting 'Yes' or 'No'. If 'Yes', include their employer's name.
- Answer whether other dependents are covered under your spouse’s or partner’s plan. If so, list the dependents' names in the provided space.
- Similarly, respond to the pharmacy coverage query for your spouse or partner, and list any covered dependents if applicable.
- Indicate whether any family member is covered by Medicare and provide the Medicare ID number and effective date if applicable.
- Answer if there are any other coverage plans outside of those previously mentioned and specify details as required.
- Review all entered information carefully for accuracy before submitting the form.
- Once the form is completed, save your changes, download a copy if needed, print it for your records, or share it as directed.
Take action now to complete your form online to ensure timely processing of your benefits.
SPRTN Customer Service 1-866-905-6146 .healthscopebenefits.com Access personal claim information, Plan SPDs, forms and general notices.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.