Loading
Get Release Of Information Authorization - West River Health Services
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Release Of Information Authorization - West River Health Services online
The Release Of Information Authorization form allows users to grant permission for their medical records to be shared with authorized parties. This guide provides step-by-step instructions to help you accurately complete the form online.
Follow the steps to successfully fill out the form.
- Use the ‘Get Form’ button to access the form and open it for editing.
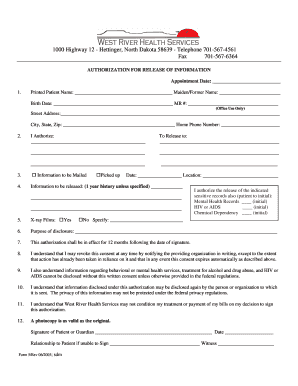
- In the first section, fill in your printed name, maiden or former name, birth date, and medical record number. This information is essential for identifying your medical records.
- Next, provide your street address, city, state, zip code, and home phone number. Ensure these details are correct for communication purposes.
- In the 'I Authorize' section, specify the name of the individual or organization you are allowing to release your information.
- In the 'To Release to' section, enter the details of the person or organization that will receive your information. Fill in the necessary fields clearly.
- Choose whether the information is to be emailed, picked up, or mailed. Select the appropriate option for your preference.
- Indicate the type of information to be released, typically covering a one-year history, or specify a different time frame if necessary.
- If applicable, initial next to any sensitive records you authorize to be released, such as mental health records, HIV/AIDS information, or chemical dependency records.
- Answer the question regarding X-ray films by selecting 'Yes' or 'No' and providing any specific details if necessary.
- Clearly state the purpose of the disclosure in the designated area. This helps clarify the reason for sharing your information.
- Review the section regarding the duration of the authorization, which is valid for 12 months unless revoked in writing.
- Acknowledge that you can revoke this authorization by notifying the organization in writing at any time.
- Be aware that certain information about behavioral or mental health services requires written consent for disclosure.
- Understand that the information may be disclosed again by the person or organization to which it is sent.
- Acknowledge that West River Health Services cannot condition your treatment or payment based on your decision to sign this authorization.
- Finally, sign and date the form. If you are a guardian signing on behalf of the patient, indicate your relationship and ensure a witness is present.
- Once all sections are completed, save your changes, download, print, or share the form as needed.
Complete your documents online efficiently and securely.
The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.