Loading
Get Claim Form Iowa Address-no Flex - M B5z
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the CLAIM FORM Iowa Address-no Flex - M B5z online
Filling out the CLAIM FORM Iowa Address-no Flex - M B5z online can be an important step in processing your health insurance claim. This guide will provide clear, step-by-step instructions to ensure you complete the form accurately and efficiently.
Follow the steps to complete the health claim form online.
- Press the ‘Get Form’ button to retrieve the claim form and open it in your preferred online editor.
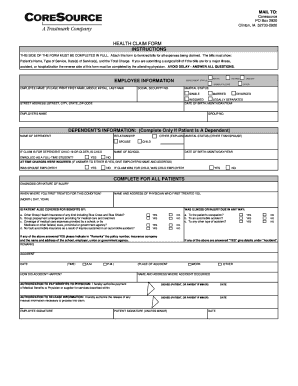
- Begin by completing the 'employee information' section. Provide your full name, social security number, employment status, marital status, and date of birth. Ensure your street address is filled out accurately, including city, state, and ZIP code.
- If applicable, complete the ‘dependent's information’ section. Include the dependent's name, relationship to you, and specify their marital status if it differs from yours. For dependent children aged 19 or older, indicate if they are enrolled as a full-time student.
- In the 'diagnosis or nature of injury' section, provide a description of the medical condition or injury. Include the name and address of the physician who treated you initially, and the date when treatment began.
- Answer the questions regarding other health insurance coverage. If applicable, provide details in the 'remarks' section about additional insurance policies or coverage that might pertain to your claim.
- Fill out the accident section if the claim is related to an accident. Provide the date, time, and location of the accident, and describe how it occurred.
- Complete the authorization sections by signing and dating the form. These signatures authorize the payment of medical benefits to your physician and the release of relevant medical information.
- Once all relevant sections are filled out, review your form to ensure accuracy. Save your changes, then choose to download, print, or share the form as needed to submit your claim.
Consider completing your health claim form online today for a more streamlined process.
Use a separate form for each family member and each physician or supplier. Enclose ORIGINAL itemized bills. Keep a copy for your records. • Mail to: Blue Cross and Blue Shield of Florida, PO Box 1798, Jacksonville, FL 32231-0014 see previous page for more instructions.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.