Get Diagnostic Assessment Program Physician Referral Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the DIAGNOSTIC ASSESSMENT PROGRAM Physician Referral Form online
Filling out the DIAGNOSTIC ASSESSMENT PROGRAM Physician Referral Form online can streamline the referral process for patients. This guide provides step-by-step instructions to ensure the form is completed accurately and efficiently, making it easier for healthcare providers and patients alike.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to access the DIAGNOSTIC ASSESSMENT PROGRAM Physician Referral Form and open it in your preferred online editor.
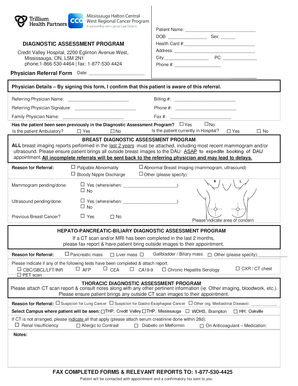
- Begin by entering the patient's full name and date of birth (DOB) in the designated fields.
- Fill in the patient's health card number, and provide their address, city, and postal code as required.
- Enter the patient's phone number to ensure correct contact details are provided.
- Date the form to indicate when it is being filled out.
- Complete the physician details section. Provide the referring physician's name, billing number, and contact phone number.
- Sign the form to confirm the patient is aware of the referral, and fill in the family physician's name and fax number.
- Indicate whether the patient has been seen previously in the diagnostic assessment program, whether they are currently hospitalized, and if they are ambulatory.
- If applicable, attach all relevant breast imaging reports from the past two years, including the most recent mammogram and/or ultrasound, for the Breast Diagnostic Assessment Program.
- Select the reason for the referral from the options listed and provide details if necessary.
- For the Hepato-Pancreatic-Biliary Diagnostic Assessment Program, attach any completed reports and indicate the reasons for referral.
- For the Thoracic Diagnostic Assessment Program, ensure that all pertinent reports are attached and specify the reason for referral.
- Finally, review all completed information before saving your changes. Download, print, or share the form as needed to finalize the referral process.
Ensure you complete the DIAGNOSTIC ASSESSMENT PROGRAM Physician Referral Form online today for a seamless referral experience.
A patient referral form is a crucial document that healthcare providers use to send patients to other specialists for further evaluation or treatment. The DIAGNOSTIC ASSESSMENT PROGRAM Physician Referral Form is designed to enhance this process by detailing patient histories and the specific reasons for referral. This form improves coordination between providers and ensures that patients receive comprehensive care.