Loading
Get Neuron Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Neuron Claim Form online
Filling out the Neuron Claim Form online can streamline the process of submitting your dental treatment claims. This guide provides clear, step-by-step instructions to help you complete the form accurately and efficiently.
Follow the steps to successfully complete your Neuron Claim Form
- Click ‘Get Form’ button to obtain the form and open it in the editor.
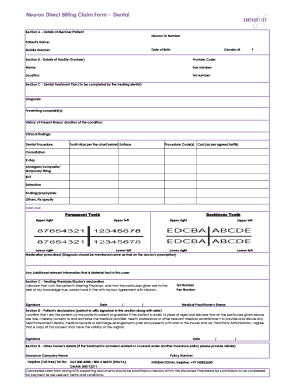
- In Section A, enter the details of the member or patient. Fill in the Neuron ID number, patient's name, date of birth, mobile number, and gender. Ensure accuracy to avoid processing delays.
- Proceed to Section B, which requires details of the facility provider. Enter the provider code, name, fax number, location, and telephone number. Accurate information is crucial for the claim processing.
- In Section C, your treating dentist will need to complete the dental treatment plan. This includes entering a diagnosis, presenting complaints, history of the present illness, clinical findings, and specific tooth-related information. They will also list the dental procedures performed along with their procedure codes and associated costs.
- Ensure to include any medications prescribed and any additional relevant information that could be vital to your case in Section C.
- The treating physician must then declare and sign in the designated area, including their contact information and medical practitioner’s stamp, confirming the accuracy of the provided details.
- The patient must affix their signature in Section D along with the date, confirming all information is truthful and consenting to necessary discussions about their treatment details.
- If applicable, fill in details about any other insurer in Section D, including the insurance company name, policy number, and helpline details.
- Once all sections are completed, review the form for accuracy. Save changes and prepare to submit your claim, ensuring it is accompanied by any required supporting documents.
Submit your completed Neuron Claim Form online today for timely processing of your dental claims.
To get your neurons working efficiently, focus on activities like regular exercise, maintaining a balanced diet, and staying mentally engaged. These practices can enhance cognitive functions and brain health. Additionally, utilizing tools like the Neuron Claim Form can streamline the process of managing your claims effectively. Remember, a healthy lifestyle promotes strong neural connections.