Loading
Get Ucare Ucare Provider Claim Reconsideration Request Form 2017-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the UCare Provider Claim Reconsideration Request Form online
Filling out the UCare Provider Claim Reconsideration Request Form online can be straightforward if you follow the right steps. This guide will provide you with detailed instructions, ensuring that you complete the form accurately and efficiently.
Follow the steps to complete your form successfully.
- Click ‘Get Form’ button to access the request form and open it in your editor.
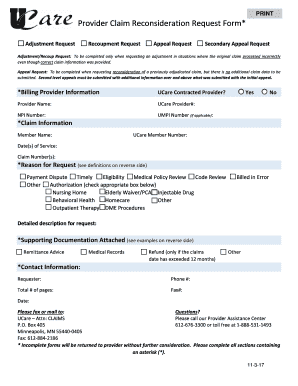
- Indicate whether you are a UCare contracted provider by selecting 'Yes' or 'No'. Fill in your provider name, UCare provider number, NPI number, and UMPI number (if applicable).
- In the Claim Information section, enter the member name and UCare member number. List the date(s) of service and the claim number(s) associated with your request.
- Select the reason for your request by checking the appropriate boxes, such as Payment Dispute, Timely, or othes. Ensure you provide a detailed description for your request in the corresponding field.
- Attach any supporting documentation required for your request. This may include remittance advice, medical records, or other relevant documents.
- Provide your contact information, including the requester's name, phone number, total number of pages, and fax number. Also, include the date of submission.
- Review your form carefully to ensure all sections marked with an asterisk (*) are completed. Incomplete forms will be returned without consideration.
- Once you have filled out the form, save your changes and proceed to download, print, or share the completed form as necessary.
Complete your UCare Provider Claim Reconsideration Request Form online today!
UCare customer service in Minnesota typically opens at 8 AM and remains available until 5 PM on weekdays. If you have queries about your plan or need assistance with claims, be sure to have the UCare Provider Claim Reconsideration Request Form handy, as it can help simplify the process and reduce waiting times.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.