Get Ny Mvft Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the NY MVFT claim form online
Filling out the NY MVFT Claim Form online can be a straightforward process when you understand each section and its requirements. This guide provides step-by-step instructions to help you complete the form accurately and efficiently.
Follow the steps to fill out the NY MVFT claim form online.
- Click the ‘Get Form’ button to obtain the form and open it in the editor.
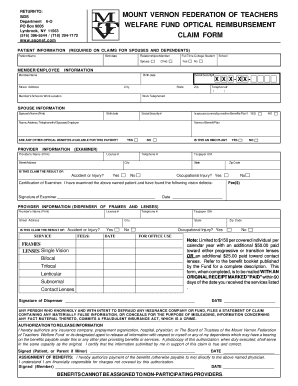
- Begin with the patient information section. Provide the patient's name, birth date, and indicate whether they are a full-time college student. If the claim is for a spouse, include their name and relationship to the member.
- In the member/employee information section, fill in the member's name, birth date, social security number, street address, city, state, zip code, and both personal and work telephone numbers.
- Complete the spouse information section if applicable. Include the spouse's name, birth date, social security number, and details about their benefits plan, including the employer's name, address, and phone number.
- If applicable, answer whether any other optical benefits are available for the patient and whether it is an HMO plan.
- Provide the provider’s information, including the provider’s name, license number, address, telephone number, and taxpayer ID number.
- Indicate whether the claim is the result of an accident, injury, or occupational injury, and include any fees for services provided, along with a signature from the examining provider.
- Complete the service section, detailing the fees for frames and lenses, while specifying the type of lenses being claimed (e.g., single vision, bifocal).
- Include the necessary signatures for both the examiner and the dispenser of frames and lenses.
- Lastly, ensure to complete the authorization to release information and assignment of benefits sections, including signatures and dates. Review the completed form carefully before saving it.
- After filling out the form, you can save changes, download, print, or share the completed NY MVFT Claim Form as needed.
Start filling out your NY MVFT claim form online today to ensure a seamless submission process.
Related links form
Deciding whether to file through your insurance or theirs often depends on the severity and specifics of the accident. If you prefer a faster resolution and your insurer covers the costs, it might be easier to go through them. However, if the other driver is fully at fault, you can explore going through their insurance instead. Regardless of your choice, remember to use the NY MVFT Claim Form to document all necessary details accurately.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.