Loading
Get First Choice Health Medical Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the First Choice Health Medical Claim Form online
Completing the First Choice Health Medical Claim Form accurately is essential for ensuring that your claims are processed efficiently. This guide offers step-by-step instructions to help you navigate the form with ease, ensuring you provide all necessary information.
Follow the steps to submit your medical claim online.
- Press the ‘Get Form’ button to access the First Choice Health Medical Claim Form and open it in your chosen editor.
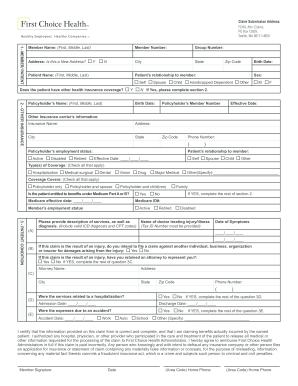
- Begin by filling in the member and patient information. Enter the member's name, including their first, middle, and last names, followed by their address. Indicate if this is a new address by selecting 'Yes' or 'No'. Provide the patient's name, member number, group number, city, state, birth date, and zip code.
- Specify the patient's relationship to the member by selecting one of the available options: 'Self', 'Child', or 'Handicapped Dependent'. Indicate the patient’s sex by checking the appropriate box for 'Male' or 'Female'. If the patient has other health insurance coverage, select 'Yes' or 'No', and if applicable, complete Section 2.
- In Section 2, provide details about the other insurance. Fill in the policyholder's name, relationship to the patient, and their effective date. Input the other insurance carrier's name, address, city, state, zip code, and phone number.
- Indicate the policyholder's employment status and the types of coverage available by checking all applicable boxes. Specify if the patient is entitled to benefits under Medicare and provide the Medicare ID and effective date, if relevant.
- In Section 3, describe the patient's condition. Provide a detailed description of services received, including valid ICD diagnosis and CPT codes. Fill in the date of symptoms onset and the name and tax ID number of the treating doctor.
- If the claim is due to an injury, indicate if you plan to file against another party and whether you have retained an attorney. If applicable, provide the attorney's contact information.
- Indicate whether the services are related to a hospitalization or accident. Fill in relevant dates and specify the circumstances of the incident, if applicable.
- Review all entries for accuracy and completeness. Sign and date the form, and provide your home phone number for contact purposes.
- Once you have completed the form, you can save changes, download, print, or share the form as needed.
Submit your completed First Choice Health Medical Claim Form online for prompt processing.
Filling out a medical authorization form starts with entering essential patient and healthcare provider information. Clearly indicate which medical records patients authorize to share and the purpose for this sharing. This detailed approach will support your First Choice Health Medical Claim Form and ensure your medical information is handled correctly.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.