Get Il Provider Information Change Request Form 2013-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the IL Provider Information Change Request Form online
Updating your practice information is essential to maintain accurate records with Blue Cross and Blue Shield of Illinois (BCBSIL). This guide will provide you with step-by-step instructions to complete the IL Provider Information Change Request Form online effectively.
Follow the steps to complete the form accurately.
- Press the ‘Get Form’ button to access the IL Provider Information Change Request Form. This will open the document in an editor where you can begin filling out your information.
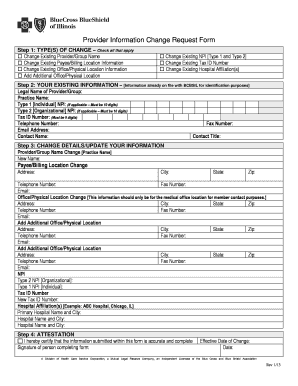
- In the first section, ‘TYPE(S) OF CHANGE,’ check all applicable boxes indicating the changes you wish to request, such as provider name, billing location, or office address.
- Next, fill out the ‘YOUR EXISTING INFORMATION’ section, including your legal name, practice name, Type 1 and Type 2 NPIs (if applicable), telephone number, fax number, email address, contact name, and contact title for identification purposes.
- In the ‘CHANGE DETAILS/UPDATE YOUR INFORMATION’ section, provide new information for each type of change you are requesting. Include updated address, telephone, fax, and email information as applicable.
- Complete the ‘ATTESTATION’ section by certifying that the information provided is accurate. Sign and date the form to confirm your submission.
- Finally, save your changes and choose to download, print, or share the completed form as necessary before submitting it to BCBSIL by mail or fax.
Begin completing the IL Provider Information Change Request Form online today to ensure your practice information is up to date!
Choosing a provider for Medicaid in Illinois can be straightforward. Start by utilizing the IL Provider Information Change Request Form to explore your options. Review the list of providers who accept Medicaid, considering factors like location, services offered, and patient reviews. This thorough approach will help you find a provider who meets your healthcare needs.