Loading
Get Kaiser Permanente 05022-005 2012-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Kaiser Permanente 05022-005 online
Filling out the Kaiser Permanente 05022-005 form online is a straightforward process that ensures your medical records are disclosed safely and efficiently. This guide provides clear, step-by-step instructions to help you complete the form accurately.
Follow the steps to complete the Kaiser Permanente 05022-005 form.
- Press the ‘Get Form’ button to access the Kaiser Permanente 05022-005 document and open it in your preferred editor.
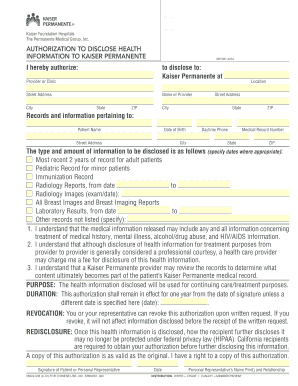
- In the section labeled 'Authorization to Disclose Health Information', fill in the name of the organization or provider you are authorizing to disclose your health information.
- Provide the details of the entity receiving the information by entering the provider or clinic name, street address, city, state, and ZIP code.
- Input your personal information in the 'Patient Name', 'Date of Birth', 'Street Address', 'City', 'State', 'ZIP', and 'Daytime Phone' fields.
- In the 'Medical Record Number' field, add your unique medical record identification, if applicable.
- Specify the type and amount of information to be disclosed by checking the relevant boxes and filling in any required dates for medical records.
- Read through the understanding sections carefully to confirm that you acknowledge the details regarding the disclosure of your health information and the limitations of such disclosure.
- Indicate the purpose of the disclosure by selecting 'continuing care/treatment purposes' or specifying another reason.
- Select the duration of the authorization by indicating that it will remain in effect for one year or provide a different date if necessary.
- Sign the form, entering the date, and if applicable, provide the name and relationship of your personal representative.
- After completing all fields, save your changes, download the document, print it for your records, or share it as needed.
Complete your Kaiser Permanente 05022-005 form online today to manage your health information effectively.
Related links form
You can efficiently request an itemized bill from Kaiser Permanente 05022-005 by using their online patient portal. Simply navigate to the billing section and follow the prompts for requesting a bill. In case you prefer speaking with someone, contact their billing support for immediate help.