Loading
Get Flex-pay Reimbursement Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Flex-Pay Reimbursement Claim form online
The Flex-Pay Reimbursement Claim form is essential for users seeking reimbursement for dependent care and medical expenses. This guide provides a clear and comprehensive overview of how to accurately complete the form online.
Follow the steps to fill out the Flex-Pay Reimbursement Claim form online.
- Click ‘Get Form’ button to access the form and open it in the editor.
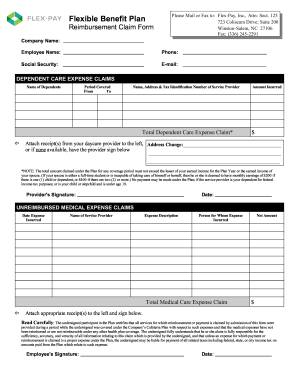
- Begin by entering your company name in the designated field. Next, fill in your name, phone number, social security number, and email address.
- For dependent care expense claims, list the names of dependents along with the period the care was provided, specifying the start and end dates.
- Provide the name, address, and tax identification number of the service provider who offered the care, followed by the total amount incurred for the service.
- Attach receipts from your daycare provider to the form. If receipts are unavailable, ensure the provider signs the form as documentation.
- For unreimbursed medical expense claims, indicate the date the expense was incurred and the name of the service provider, along with a brief description of the expense.
- Specify the person for whom the medical expense was incurred, complete the total medical care expense claim, and include the net amount being claimed.
- Attach appropriate medical receipts to the form. Then, read the certification statement carefully before signing and dating the form.
- Finally, review all entries for accuracy and completeness before saving your changes. You may then download, print, or share the completed form as needed.
Complete your Flex-Pay Reimbursement Claim form online today to ensure timely processing of your claims.
Related links form
To make a reimbursement form, you can use various templates available online, including those from uslegalforms. Begin by filling out all relevant information about your expenses clearly and accurately. After drafting your form, double-check that it includes any required documentation, such as receipts, to streamline processing.