Loading
Get Subscriber Submit Claim Form - Bu
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the SUBSCRIBER SUBMIT CLAIM FORM - Bu online
Filling out the SUBSCRIBER SUBMIT CLAIM FORM - Bu online can seem daunting, but with the right guidance, you can complete the process smoothly. This guide provides a step-by-step approach to ensure all necessary information is accurately submitted.
Follow the steps to successfully complete your claim form.
- Click ‘Get Form’ button to obtain the form and open it in your preferred editing tool.
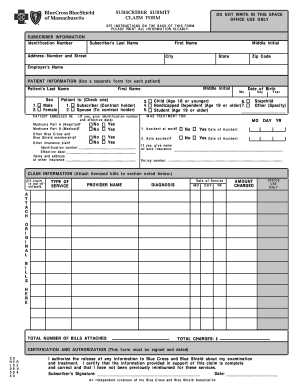
- Begin by entering your subscriber information. Provide your identification number, last name, first name, middle initial, and full address, including city, state, and zip code.
- Next, fill out the patient information. Indicate the patient's last name, first name, middle initial, date of birth, and sex. Check the appropriate box to specify the patient's relationship to the subscriber.
- Indicate if the patient received any treatment under Medicare Part A or Part B and if there were any accidents leading to the treatment. If 'Yes,' provide the necessary details.
- Complete the claim information section by listing the type of service, provider name, date of service, diagnosis, and amount charged. Ensure to attach itemized bills that include all required details.
- In the certification and authorization section, sign and date the form, certifying the completeness and accuracy of the information provided.
- Finally, review your completed form against the claim checklist included in the instructions. Ensure all necessary documentation is attached before submission.
- Once satisfied with your submission, save changes, download the form for your records, and prepare to mail it to the specified address.
Start filling out your SUBSCRIBER SUBMIT CLAIM FORM - Bu online today!
BCBS FEP: 1-800-411-BLUE (2583) BCBS FEP Dental: 1-855-504-BLUE (2583) BCBS FEP Vision: 1-888-550-BLUE (2583)
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.