Loading
Get Wi F-80983 2019-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WI F-80983 online
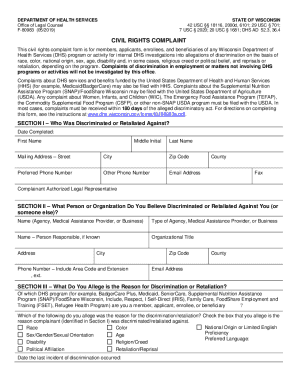
The WI F-80983 form is a civil rights complaint document utilized by individuals seeking to report discrimination or retaliation within Wisconsin Department of Health Services programs. This guide offers step-by-step instructions aimed at simplifying the process of completing the form online.
Follow the steps to accurately complete the WI F-80983 form online.
- Press the ‘Get Form’ button to download the form and open it in your preferred electronic editor.
- Begin by completing Section I, which asks for the details of the individual who has faced discrimination or retaliation. Fill in your first name, middle initial, last name, mailing address, city, zip code, preferred phone number, other phone number, email address, and county.
- In Section II, provide the name of the person or organization you believe has discriminated against you. This includes filling in their type (agency, medical assistance provider, or business) and, if known, the name and title of the responsible person along with their contact information.
- Proceed to Section III. Here, indicate the program you are associated with and identify the reason for the reported discrimination or retaliation by checking the appropriate box or boxes.
- In Section IV, describe the discriminatory or retaliatory actions that occurred. Be specific — include dates of actions and the names of individuals involved. Explain why you believe these actions were discriminatory based on the reasons checked in Section III.
- Finally, in Section V, submit your complaint by mailing or emailing the completed form to the Department of Health Services' Civil Rights Compliance Office according to the provided contact details.
- After reviewing your form for accuracy, you can save your changes, download a copy for your records, print the form, or share it as needed.
Complete your WI F-80983 form online today to ensure your civil rights complaint is addressed.
The Elder Law Center of the Coalition of Wisconsin Aging Groups - Phone: 608-224-0660. U.S. Equal Employment Opportunity Commission - Phone: 414-297-1111, 414-297-1115 (TTY) Job Accommodations Network (JAN) - Phone: 800-526-7234 (Voice/TTY)