Loading
Get Canada Scarborough Health Network Centralized Intake Mental Health Outpatient Programs Referral Form 2020-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Canada Scarborough Health Network Centralized Intake Mental Health Outpatient Programs Referral Form online
Filling out the Canada Scarborough Health Network Centralized Intake Mental Health Outpatient Programs Referral Form online can be a straightforward process when approached with clear guidance. This comprehensive guide offers step-by-step instructions to ensure that all necessary information is accurately provided for effective processing of your referral.
Follow the steps to successfully complete the referral form.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Begin by entering the date in the specified field, ensuring to use the correct format.
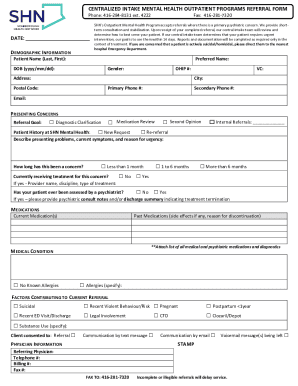
- Fill in the demographic information section, including the patient’s name (last and first), preferred name, date of birth, gender, OHIP number, address, city, postal code, primary phone number, secondary phone number, and email.
- In the presenting concerns section, check all relevant boxes to indicate the nature of the referral, including diagnostic clarification, medication review, or second opinion.
- Indicate whether this is a new request or a re-referral and fill in any internal referrals if applicable.
- Clearly articulate the referral goal and describe the presenting problems, current symptoms, and urgency, noting the timeline of concern.
- If the patient is currently receiving treatment, provide the name, discipline, and type of treatment for the provider.
- Indicate whether the patient has ever been assessed by a psychiatrist, and provide relevant psychiatric consult notes if available.
- List current medications and any past medications along with side effects and reasons for discontinuation. Attach a comprehensive list of all relevant medications and diagnostics.
- Note any known medical conditions or allergies and provide specific details if applicable.
- Indicate any factors contributing to the current referral by checking relevant boxes such as suicidal risk, recent emergency department visit, or legal involvement.
- Complete the physician information section, including the referring physician's name, telephone number, billing number, and fax number.
- Ensure to review all provided information for completeness and legibility, as incomplete referrals may delay service.
- Once all sections are completed, save changes, and prepare to download, print, or share the form.
Complete your referral form online today to ensure timely access to mental health services.
Related links form
An Assertive Community Treatment (ACT) team consists of a community-based group of medical, behavioral health and rehabilitation professionals who use a team approach to meet the needs of an individual with severe and persistent mental illness.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.