Loading
Get Form Instructions Pdf - 69 Kb - Cdc
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to use or fill out the Form Instructions PDF - 69 KB - Cdc online
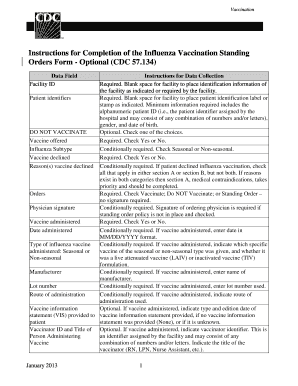
This guide provides detailed instructions on completing the Influenza Vaccination Standing Orders Form as outlined in the Form Instructions PDF. By following these steps, users can effectively fill out the required fields to ensure accurate documentation.
Follow the steps to successfully complete the form online.
- Press the ‘Get Form’ button to acquire the form and open it for editing.
- Enter the facility ID in the designated area to record the identification information of your facility.
- Attach patient identifiers by placing the patient identification label or stamp in the required space. Ensure to include the alphanumeric patient ID, gender, and date of birth.
- In the 'DO NOT VACCINATE' section, make your selection by checking the appropriate option.
- For the vaccine offered field, indicate your response by checking Yes or No.
- In the Influenza subtype section, conditionally check either Seasonal or Non-seasonal as required.
- If the vaccine is declined, mark Yes or No accordingly.
- If the vaccine is declined, identify the reasons in Section A or Section B, ensuring that if both apply, you complete Section A first.
- In the Orders section, mark your decision: Vaccinate, Do NOT Vaccinate, or Standing Order – no signature required.
- If no standing order policy is in place, the physician’s signature is conditionally required. Make sure to sign if applicable.
- Mark whether the vaccine was administered by checking Yes or No.
- If administered, enter the date of vaccination in MM/DD/YYYY format.
- Indicate the type of influenza vaccine administered, specifying if it was Seasonal or Non-seasonal.
- If applicable, record the name of the vaccine manufacturer.
- Document the lot number used if the vaccine was administered.
- Specify the route of administration if the vaccine was given.
- If the vaccine was administered, indicate the type and edition date of the vaccine information statement provided.
- Optionally, indicate the vaccinator ID and their title (e.g., RN, LPN) if applicable.
- If necessary, include the name of the vaccinator in the format of last name, first name, middle name, or initial.
- Optional: Provide the work address, city, state, and zip code of the vaccinator.
- Once all fields are completed, save changes, download, print, or share the form as required.
Complete your documents online with confidence and accuracy.
OSHA regulations require that workplaces provide employees respirator training prior to use in the workplace. It is important that you know what respirator to use and how to use it correctly so that it can provide the expected protection. Refer to OSHA 29 CFR 1910.134external icon for more information.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.