- US Legal Forms
- Form Library
- More Forms
- More Multi-State Forms
- IL HSHS Medical Group Authorization For Release Of Confidential Health Information 2011
Get IL HSHS Medical Group Authorization For Release Of Confidential Health Information 2011-2024
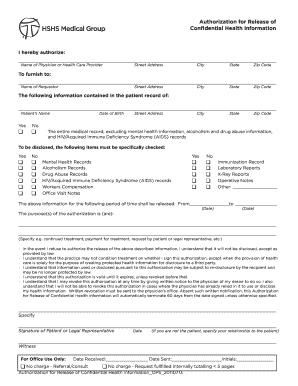
H Care Provider Street Address City State Zip Code To furnish to: Name of Requestor Street Address City State Zip Code The following information contained in the patient record of: Patient s Name Yes q No q Date of Birth Street Address City State Zip Code The entire medical record,.
How It Works
-
Open form follow the instructions
-
Easily sign the form with your finger
-
Send filled & signed form or save
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Excluding FAQ
-
The Illinois Hospital Licensing Act requires that medical records be maintained on every patient ing to hospital policy and for a period of not less than ten years.
-
“Retain three (3) years in office, and then transfer to the Illinois State Archives for permanent retention.” NOTE: The term “permanent,” when used for archival and retention purposes, means forever. Using the term permanent to define a record's retention means that it has lasting value.
-
There is no specific rule for how long doctors in Illinois must keep medical records. You have the right to see, get a copy of, and amend your medical record for as long as your health care provider has it. You have the right to see your medical record. You also have the right to get a copy of your medical record.
-
You can submit your medical records request via email or mail to the hospital from which you're seeking the records. If you send via mail, please address the envelope to the attention of the Health Information Management Department at the hospital.
-
A HIPAA release form is a document that – when signed – allows healthcare providers to share a patient's protected health information (PHI) with specified individuals or organizations, ing to the details stipulated in the form.
-
The Rules for the Health Insurance Portability and Accountability Act (“HIPAA”) require that records be maintained for a minimum of 6 years from the date of their creation and that records of any disclosure be maintained for 6 years from the disclosure date.
-
ing to the HIPAA laws, health records must be kept for fifty years after a person is dead. However, some states only have a five to ten years retention period.
-
NOTICE: Requests for vital records may be submitted to the IDPH Division of Vital Records via regular mail. Be advised that the processing time for requests is approximately 12 weeks from the time your paperwork is received.
Referral Related content
-
My SIU - SIU School of Medicine
The my.siumed.edu portal provides links that are restricted or relevant to School of...
Learn more -
REGISTER RULES
by R RULES · Cited by 1 — ADOPTED RULES. COMMERCE COMMISSION, ILLINOIS. Approval of...
Learn more -
RESIDENT AND FELLOW MANUAL 2017
Mar 17, 2017 — • Release of medical information may be made without a patient's...
Learn more -
MIDWEST TECHNICAL INSTITUTE STUDENT CATALOG
Each student's identity will be maintained in a format designed to preserve privacy as...
Learn more -
Radiation Therapy Program Student Handbook
required to complete and sign the authorization, acknowledgement, and release form that...
Learn more -
Dietetic Internship Program
by IL CARBONDALE · Cited by 22 — information, not be disclosed absent a written...
Learn more -
July-2019-Nursing-Guide.pdf
Jul 7, 2019 — CONFIDENTIALITY OF PROTECTED HEALTH INFORMATION ... Refusal to sign the...
Learn more -
catalog0809.pdf
The catalog is not to be considered a binding contract. The College reserves the right to...
Learn more -
Case 1:21-cv-00081-SEB-MJD Document 18 Filed...
UNITED STATES DISTRICT COURT. FOR THE SOUTHERN DISTRICT OF INDIANA. INDIANAPOLIS DIVISION...
Learn more -
AGENDA MEETING OF THE BOARD OF TRUSTEES OF ...
Apr 1, 2022 — Chair Gilbert called the meeting to order. The following members of the...
Learn more -
Radiation Therapy Program Student Handbook
Section B- Program...
Learn more -
ILLINOIS Din Mee EASTERN BOARD MONTH Ma L Olney C...
Medical Assistant (LTC) – Clay County Health Medical Clinic – Flora. Medical...
Learn more -
2009-2011 GRAdUATE CATALOG
This catalog was prepared based on the best information available at the time. The...
Learn more -
2009-2011 UNDERGRADUATE CATALOG
This catalog was prepared based on the best information available at the time. The...
Learn more -
July-2021-Nursing-Guide-FINAL- ...
Since 1909, we have been educating students for healthcare professions. Our array of...
Learn more -
July-2019-Nursing-Guide.pdf
Jul 7, 2019 — Confidentiality of Protected Health Information. Clinical experience...
Learn more -
Case 1:21-cv-00081-SEB-MJD Document 18 Filed...
UNITED STATES DISTRICT COURT. FOR THE SOUTHERN DISTRICT OF INDIANA. INDIANAPOLIS DIVISION...
Learn more -
Sc cho ol o of N Nur rsin ng
Faculty must complete the Authorization for Release of Information form prior to hire...
Learn more -
Curriculum Vitae Jamila M. Torain, Ph.D.
by J Torain · 2019 — University of Maryland, School of Medicine Graduate School...
Learn more -
2013-2014 Catalog
Jan 1, 2013 — College of Southern Idaho 733-9554. College of Southern Idaho toll free...
Learn more -
I-CARE - Illinois Department of Public Health
The application allows public and private healthcare providers to share the immunization...
Learn more -
MACON COUNTY CARE COORDINATION
... release of information forms permitting disclosure of medical and/or behavioral health...
Learn more -
REGISTER RULES
by R RULES · Cited by 1 — ADOPTED RULES. COMMERCE COMMISSION, ILLINOIS. Approval of...
Learn more -
Lab Pays $16500 Settlement to HHS, Resolving...
Jan 3, 2023 — Life Hope Labs agreed to implement a corrective action plan and pay...
Learn more -
Template Document for Orders and whatnot
Dec 21, 2012 — needed to move medical images); Letter from David LaFuria, Counsel for...
Learn more -
RFP: City of Chicago Deferred Compensation Plan
... Group accounts aaaccoaccouins. d. Other (provide details). Total, 100%, 100%. 6...
Learn more -
Rural Health Clinics
This is a data file containing 7 calendar years of 2567 Statement of Deficiency text...
Learn more -
CONTROLLED SUBSTANCES BOARD Room N208, 4822 ...
Jan 10, 2020 — CONTROLLED SUBSTANCES BOARD. Room N208, 4822 Madison Yards Way, 2nd...
Learn more -
2019 Illinois Session Laws
Effective Date of Laws. The General Assembly shall provide by law for a uniform effective...
Learn more -
9-21-2020 Council Meeting Agenda pages 18 to 184
Sep 15, 2020 — Occupational Health experience through HSHS; improved use of Nurse Case...
Learn more -
My SIU - SIU School of Medicine
The my.siumed.edu portal provides links that are restricted or relevant to School of...
Learn more -
hospital sisters health system
Health-Related Records: SIU shall, as part of its curriculum, instruct students as to the...
Learn more -
REGISTER RULES
by R RULES · Cited by 1 — ADOPTED RULES. COMMERCE COMMISSION, ILLINOIS. Approval of...
Learn more -
July-2021-Nursing-Guide-FINAL- ...
Confidentiality of Protected Health Information. Clinical experience requires students to...
Learn more -
Radiation Therapy Program Student Handbook
C-11 Policy in Regard to Records and Release of Information. 1. The release ... Marshfield...
Learn more -
Case 1:21-cv-00081-SEB-MJD Document 18 Filed...
UNITED STATES DISTRICT COURT. FOR THE SOUTHERN DISTRICT OF INDIANA. INDIANAPOLIS DIVISION...
Learn more -
MIDWEST TECHNICAL INSTITUTE STUDENT CATALOG
o Prospective students will be required to meet the standards of the Illinois Healthcare...
Learn more -
ILLINOIS Din Mee EASTERN BOARD MONTH Ma L Olney C...
prevent use or disclosure of Protected Health Information other than as permitted by this...
Learn more -
Dietetic Internship Program
by IL CARBONDALE · Cited by 22 — information, not be disclosed absent a written...
Learn more -
Minutes of the meetings of the BOARD OF TRUSTEES...
Mar 15, 2022 — of the Corporation's confidential information, other than for the benefit...
Learn more -
I-CARE - Illinois Department of Public Health
The application allows public and private healthcare providers to share the immunization...
Learn more -
MACON COUNTY CARE COORDINATION
... authorization for release of information forms, enter key ... forms permitting...
Learn more -
REGISTER RULES
by R RULES · Cited by 1 — ADOPTED RULES. COMMERCE COMMISSION, ILLINOIS. Approval of...
Learn more -
RFP: City of Chicago Deferred Compensation Plan
... information, as described in Section 2.11 of this Agreement. If the City, by ... form...
Learn more -
Informed Consent FAQs
The informed consent process involves three key features: (1) disclosing to potential...
Learn more -
CONTROLLED SUBSTANCES BOARD Room N208, 4822 ...
Jan 10, 2020 — CONTROLLED SUBSTANCES BOARD. Room N208, 4822 Madison Yards Way, 2nd...
Learn more -
Template Document for Orders and whatnot
Dec 21, 2012 — needed to move medical images); Letter from David LaFuria, Counsel for...
Learn more -
Rural Health Clinics
This is a data file containing 7 calendar years of 2567 Statement of Deficiency text...
Learn more -
0001071000-02-000003.txt
... information statements incorporated by reference in Part III of this Form 10-K or any...
Learn more -
9-21-2020 Council Meeting Agenda pages 18 to 184
Sep 15, 2020 — Occupational Health experience through HSHS; improved use of Nurse Case...
Learn more -
MACON COUNTY CARE COORDINATION
... release of information forms permitting disclosure of medical and/or behavioral health...
Learn more -
Application 1/12/2018
Jan 12, 2018 — i ant s Provide for each applicant refer to Part 1130.220. Exact Legal...
Learn more -
FCC-12-150A1.txt
... health information exchange, remote training, and other telehealth applications....
Learn more -
RFP: City of Chicago Deferred Compensation Plan
... Health Insurance Portability and Accountability Act, the Health Information Technology...
Learn more -
2019 Illinois Session Laws
Effective Date of Laws. The General Assembly shall provide by law for a uniform effective...
Learn more -
Rural Health Clinics
This is a data file containing 7 calendar years of 2567 Statement of Deficiency text...
Learn more -
Contract By Authorized Board
Mar 15, 2018 — This Contract is entered into by and between the State of Wisconsin...
Learn more -
House Members Bill List Report
Andersson, Steven A. Bill #, ABR - Short Description, Chamber, Last Action, Last Action...
Learn more -
0001071000-02-000003.txt
... release of the mortgage interest following payoffs of residential mortgage loans and...
Learn more -
VIRTUAL/TELECONFERENCE BOARD OF NURSING Virtual...
Apr 14, 2022 — medical records and other health information. Patients can expect...
Learn more -
21 Compliance Report (Illinois Department of...
maintenance, and exchange of confidential personal and medical information ... The...
Learn more -
MACON COUNTY CARE COORDINATION
... release of information forms permitting disclosure of medical and/or behavioral health...
Learn more -
_
Exchange of EHRs avoids duplicative medical tests and errors in prescriptions, and gives...
Learn more -
queryResult
Records for all inquiries made to AskCVM mailbox for the year 2019, including log...
Learn more -
Contract By Authorized Board
15 Mar 2018 — This Contract is entered into by and between the State of Wisconsin, Group...
Learn more -
Rural Health Clinics
This is a data file containing 7 calendar years of 2567 Statement of Deficiency text...
Learn more -
RFP: City of Chicago Deferred Compensation Plan
... Medical Practice Groups. Exhibit X: Agencies' List of Medical Services...
Learn more -
0001071000-02-000003.txt
... information statements incorporated by reference in Part III of this Form 10-K or any...
Learn more -
—Tony Kurtz— - Wisconsin Legislative Documents
20 Jan 2022 — It is information that has been largely kept confidential by health...
Learn more -
House Members Bill List Report
Andersson, Steven A. Bill #, ABR - Short Description, Chamber, Last Action, Last Action...
Learn more -
Radiation Therapy Program Student Handbook
required to complete and sign the authorization, acknowledgement, and release form that...
Learn more -
2009-2011 GRAdUATE CATALOG
This catalog was prepared based on the best information available at the time. The...
Learn more -
2009-2011 UNDERGRADUATE CATALOG
This catalog was prepared based on the best information available at the time. The...
Learn more -
Sc cho ol o of N Nur rsin ng
Faculty must complete the Authorization for Release of Information form prior to hire....
Learn more -
July-2019-Nursing-Guide.pdf
Jul 7, 2019 — CONFIDENTIALITY OF PROTECTED HEALTH INFORMATION ... Refusal to sign the...
Learn more -
Table of Contents
... medicine, dentistry, veterinary medicine or complete graduate degrees in microbiology...
Learn more -
Meeting of the Board of Trustees Monday, June 27...
Jun 27, 2011 — Any writings relating to open session agenda items and distributed to all...
Learn more -
2016 | 2017 Academic Year
GRADUATE DEGREES. Doctor of Education in Organizational Leadership. Doctor of Physical...
Learn more -
Curriculum Vitae Jamila M. Torain, Ph.D.
by J Torain · 2019 — University of Maryland, School of Medicine Graduate School...
Learn more -
July-2021-Nursing-Guide-FINAL- ...
CONFIDENTIALITY OF PROTECTED HEALTH INFORMATION ... Refusal to sign the consent to release...
Learn more
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.
Keywords relevant to IL HSHS Medical Group Authorization For Release Of Confidential Health Information
- notication
- specically
- revocation
- totalling
- Immunization
- Pursuant
- excluding
- referral
- revoke
- provision
- disclosed
- alcoholism
- specify
- furnish
- relied
USLegal fulfills industry-leading security and compliance standards.
-

VeriSign secured
#1 Internet-trusted security seal. Ensures that a website is free of malware attacks.
-

Accredited Business
Guarantees that a business meets BBB accreditation standards in the US and Canada.
-

TopTen Reviews
Highest customer reviews on one of the most highly-trusted product review platforms.

