Loading
Get Wellspan Occupational Health Employer Authorization Form 2016-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WellSpan Occupational Health Employer Authorization Form online
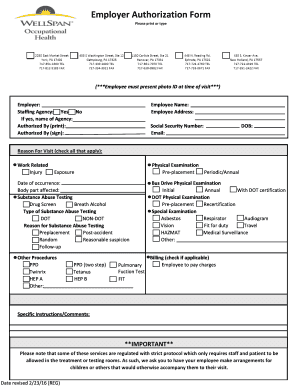
Filling out the WellSpan Occupational Health Employer Authorization Form online may seem daunting, but understanding each section can make the process smoother. This guide provides clear, step-by-step instructions for successfully completing the form while ensuring all necessary information is captured accurately.
Follow the steps to complete the form effectively.
- Press the ‘Get Form’ button to access the form and open it in your editing tool.
- Enter the employer's name in the designated field at the top of the form.
- Indicate whether the employee is from a staffing agency by selecting 'Yes' or 'No.' If 'Yes,' provide the name of the agency.
- In the 'Authorized By' section, print and sign the name of the authorized individual.
- Fill in the employee's name and address in the appropriate fields.
- Provide the employee's social security number, email, and date of birth.
- Select the reason for the visit by checking all applicable boxes, such as 'Work Related,' 'Physical Examination,' or 'Substance Abuse Testing.' Be sure to include any relevant details, such as the date of occurrence and affected body part for injuries.
- If applicable, fill in details regarding substance abuse testing. Specify the type (DOT or Non-DOT) and the reason for testing.
- Complete any additional procedures that apply, including immunizations or specialized tests.
- If required, indicate if the employee is responsible for paying charges by checking the billing box.
- Finally, include any specific instructions or comments in the designated area.
- Review all entries for accuracy, then save changes, download, print, or share the completed form as needed.
Complete your forms online today for an efficient and streamlined process!
Related links form
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.