Loading
Get Il Edward-elmhurst Health Authorization To Use And Disclose Health Information 2021-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the IL Edward-Elmhurst Health Authorization To Use And Disclose Health Information online
This guide will help you navigate the process of completing the IL Edward-Elmhurst Health Authorization To Use And Disclose Health Information form online. The form is essential for permitting the sharing of your health information with designated individuals or organizations.
Follow the steps to complete the form successfully.
- Press the ‘Get Form’ button to access the authorization form and open it in your preferred digital format.
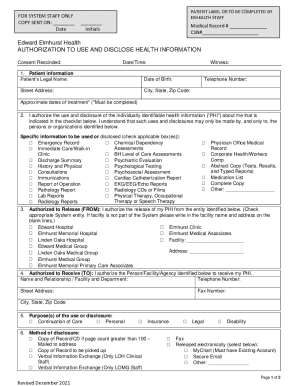
- Begin by filling out the patient information section with the patient's legal name, date of birth, address, telephone number, and approximate dates of treatment.
- In the next section, authorize the use and disclosure of specific health information by checking the relevant boxes corresponding to the types of records you would like to disclose.
- Identify the organization or entity from which the health information is being released by selecting from the provided options. If applicable, fill in the name and address of any facility not included in the list.
- Indicate who is authorized to receive your health information by providing their name, relationship, facility name, address, and contact details.
- Select the purpose(s) for the use or disclosure of the health information from the available options.
- Choose the preferred method of disclosure, selecting options for how you would like to receive your information.
- Review and acknowledge your understanding of the terms outlined in the authorization form. It's important to comprehend your rights regarding the use and protection of your health information.
- Sign and date the form, ensuring that if applicable, you also include the required signatures of legal representatives or witnesses.
- Once completed, you can save the changes to the form, download it for your records, print a physical copy, or share it as needed.
Start completing your documents online today!
You can also send them to Edward HIM/Medical Records Department, 801 S. Washington Street, Naperville, IL 60540, fax to 331-221-2390 or email to mychart.activation@eehealth.org.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.