Loading
Get Ca Preferred Ipa Referral/authorization Request 2016-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CA Preferred IPA Referral/Authorization Request online
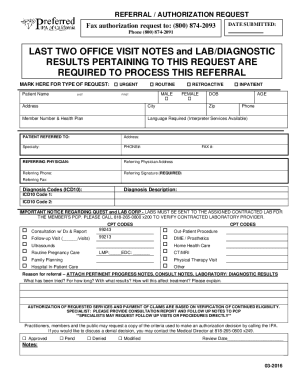
Completing the CA Preferred IPA Referral/Authorization Request is essential for ensuring timely referrals and authorizations within the healthcare system. This guide provides clear, step-by-step instructions to assist users in filling out the form accurately and efficiently online.
Follow the steps to complete your referral and authorization request.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Begin by entering the date submitted in the provided field at the top of the form.
- Indicate the type of request by marking one of the options: urgent, routine, or retroactive.
- Fill in the patient’s last and first name along with their date of birth, age, and address, including city and zip code.
- Input the member number and health plan details.
- Specify if a language interpreter is required by indicating your needs in the designated area.
- Complete the information for the patient being referred, including their address, specialty, and phone number.
- Record the details of the referring physician, including their name, address, phone number, and fax number.
- Sign in the required field to validate the referral and authorization request.
- Input the diagnosis codes (ICD10) and descriptions as needed in the respective fields.
- Select the appropriate CPT codes for the services being requested and provide any necessary details regarding the procedure.
- Include a reason for referral, attaching any pertinent progress notes, consult notes, or laboratory results.
- Ensure that you have answered the questions about prior treatments and their outcomes to provide a comprehensive view of the patient's history.
- Review all the filled information to ensure accuracy before finalizing the form.
- Save your changes, and utilize the options to download, print, or share the completed form as necessary.
Ensure your referrals and authorizations are processed smoothly by completing the CA Preferred IPA Referral/Authorization Request online today.
The form a provider uses to request authorization is called a Prior Authorization (PA).