Loading
Get Or Careoregon Pharmacy Provider Reconsideration Request Form 2016
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the OR CareOregon Pharmacy Provider Reconsideration Request Form online
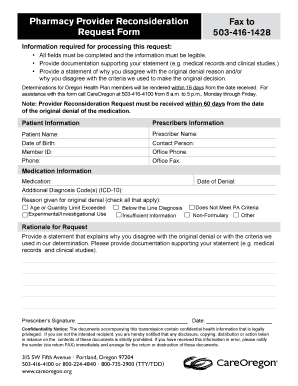
Filling out the OR CareOregon Pharmacy Provider Reconsideration Request Form online can be straightforward with the right guidance. This form is essential for requesting a review of a medication denial, ensuring all necessary information is clearly provided to facilitate the reconsideration process.
Follow the steps to complete your request effectively.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Complete the patient information section, including the patient’s name, date of birth, and member ID. Make sure all entries are legible to avoid processing delays.
- Provide the contact person's details by entering their name, office phone number, and office fax number. This information ensures that CareOregon can reach someone for follow-up.
- Indicate the date of the original denial in the designated field. This helps in tracking the request timeframe.
- List any additional diagnosis codes (ICD-10) that apply to the situation, ensuring accurate documentation is provided.
- Check all applicable reasons given for the original denial. Options include age or quantity limit exceeded, experimental/investigational use, below the line diagnosis, insufficient information, does not meet PA criteria, non-formulary, or other.
- Provide a comprehensive statement explaining why you disagree with the original denial reason and/or the criteria used, along with any supporting documentation like medical records or clinical studies.
- The prescriber should sign and date the form in the designated areas. This signifies the prescriber's agreement and authorization for the request.
- Once all sections are completed, save your changes and prepare to submit the form. You can download, print, or share the form as needed before faxing it to 503-416-1428.
Complete your documents online to expedite the reconsideration process.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
When submitting claims to CareOregon, you have two options: Send claims electronically using our payer ID 93975.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.