Loading
Get Guardian - Notice And Proof Of Claim For Disability Benefits
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Guardian - Notice And Proof Of Claim For Disability Benefits online
Completing the Guardian - Notice And Proof Of Claim For Disability Benefits can seem daunting, but this guide will break down each section to ensure you fill out the form correctly and completely. By following these steps, you can streamline the process of claiming your disability benefits.
Follow the steps to complete the form successfully.
- Use the ‘Get Form’ button to access the Guardian - Notice And Proof Of Claim For Disability Benefits form in your online editor.
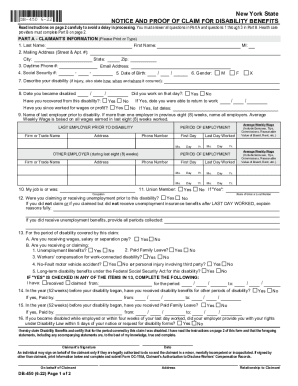
- In Part A, enter the claimant's information. Fill in your last name, first name, middle initial, mailing address, city, state, ZIP code, and daytime phone number. Ensure that these details are accurate for effective communication.
- Provide your email address and social security number. Include your date of birth in the specified format. Select your gender and describe your disability thoroughly, detailing circumstances such as how, when, and where the injury occurred.
- Indicate the date you became disabled and whether you have recovered. Answer whether you worked on the day of your disability and, if applicable, provide the date you were able to return to work.
- List your last employer prior to your disability. If you had multiple employers in the last eight weeks, include all relevant details such as the firm name, address, employment periods, and phone number.
- Provide information regarding your occupation, union membership (if applicable), and your average weekly wage, including any bonuses or additional income.
- Answer the section regarding any unemployment claims made prior to your disability. Provide the reasons if you did not receive unemployment benefits.
- Complete inquiries regarding any other benefits you may be receiving or have claimed for your disability. Fill these out as applicable.
- After filling out all sections of Part A, you will need to sign and date the form to certify your claim. Ensure that all information is accurate.
- In Part B, the health care provider must complete their section regarding your diagnosis and treatment. Ensure that they return this completed form to you within the stipulated time frame.
- Review the entire form for completeness and accuracy before submission. Once finalized, save your changes, and you can download or print your completed form for submission.
Start filling out your Guardian - Notice And Proof Of Claim For Disability Benefits online today for a seamless process!
Elimination Periods and Long-Term Care Insurance Most policies require policyholders to need consecutive days of services or disability. For example, if your elimination period was 90 days, you would need to be in a hospital or disabled for 90 consecutive days before any coverage begins.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.