Loading
Get Memorialcare Referral Authorization Request Form 2016-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MemorialCare Referral Authorization Request Form online
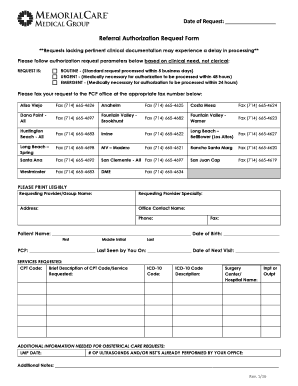
The MemorialCare Referral Authorization Request Form is essential for initiating the referral process for healthcare services. This guide provides clear and supportive instructions on how to fill out this form efficiently and accurately online.
Follow the steps to complete the MemorialCare Referral Authorization Request Form online
- Press the ‘Get Form’ button to access the MemorialCare Referral Authorization Request Form and open it in your chosen editor.
- Fill in the ‘Date of Request’ at the top of the form to indicate when the request is being made.
- Select the appropriate request type by checking one of the three boxes: Routine, Urgent, or Emergent, based on the clinical need.
- Provide the ‘Requesting Provider/Group Name’ and specialty to identify the healthcare provider making the referral.
- Input the office contact information, including the name, phone number, and fax number where the authorization can be sent.
- Enter the patient’s details: full name, date of birth, and primary care provider's name along with their last visit date.
- Complete the ‘Services Requested’ section by including the CPT code with a brief description and the corresponding ICD-10 code with its description.
- Specify the surgery center or hospital name and indicate whether the service is for inpatient or outpatient care.
- If applicable, provide additional information for obstetrical care requests, including the Last Menstrual Period (LMP) date and any ultrasounds or NSTs performed.
- Use the section for additional notes to include any relevant information that may assist in processing the request.
- After entering all required information, save your changes, then download, print, or share the completed form as necessary.
Complete your MemorialCare Referral Authorization Request Form online today!
Related links form
Claims Address: PO BOX 20900 Fountain Valley, CA 92708 1-855-367-7747 Fax: (657) 241-3960 Monday thru Friday: 8 a.m. to 5 p.m.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.