Loading
Get Piedmont Healthcare Authorization For The Use And Disclosure Of Protected Health Information 2014-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Piedmont HealthCare Authorization For The Use And Disclosure Of Protected Health Information online
Navigating the process of completing the Piedmont HealthCare Authorization For The Use And Disclosure Of Protected Health Information online can seem daunting. This guide provides clear, step-by-step instructions to help you fill out the form accurately and efficiently.
Follow the steps to complete the form online:
- Press the ‘Get Form’ button to access the document and open it in the online editor.
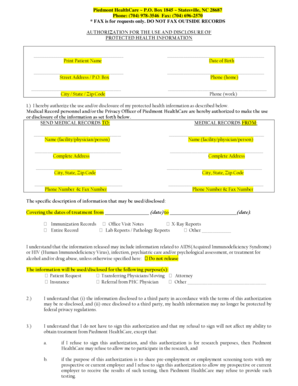
- Begin by entering the patient's full name in the designated field labeled 'Print Patient Name'.
- Next, fill in the date of birth in the section labeled 'Date of Birth'.
- Provide the patient’s complete street address or P.O. Box in the 'Street Address / P.O. Box' section.
- In the 'Phone (home)' field, input the patient’s home phone number.
- Complete the 'City / State / Zip Code' fields with the patient’s city, state, and zip code.
- Fill in the 'Phone (work)' field with the patient’s work phone number.
- Authorize the use or disclosure of protected health information by stating the name of the person, facility, or physician who will receive the records.
- In the 'SEND MEDICAL RECORDS TO:' section, provide the full name and address of the recipient.
- Describe the information to be disclosed by checking the relevant boxes such as immunization records or lab reports.
- Indicate the dates of treatment from the specified start date to end date within the section provided.
- If applicable, specify if there are any restrictions on the release of sensitive information, such as AIDS or substance abuse treatment.
- State the purpose for which the information will be disclosed by checking the appropriate box or writing in a custom purpose.
- Acknowledge the understanding of re-disclosure by reading the paragraph and confirming agreement.
- Understand that signature authorization is not mandatory and fill out the relevant details if applicable.
- Provide the expiration date for the authorization; if left blank, it will automatically expire in ninety days.
- Sign the document with the signature of the patient or their personal representative, followed by the date.
- If signing as a representative, check the appropriate legal authority and include supporting legal documents if needed.
- Once completed, ensure to save changes, download a copy, print the document, or share it as needed.
Fill out your Piedmont HealthCare Authorization For The Use And Disclosure Of Protected Health Information online today.
Related links form
If the data in question meet the definition of PHI and are being used for purposes that fall within HIPAA's definition of research, HIPAA generally requires explicit written authorization (consent) from the data subject for research uses.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.