Loading
Get Hhs Cms-1490 (formerly Cms-1490s) 2005
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the HHS CMS-1490 (Formerly CMS-1490S) online
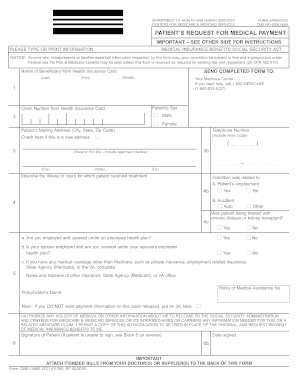
The HHS CMS-1490 (Formerly CMS-1490S) is a crucial form for individuals seeking medical payment from Medicare. This guide will help you complete the form accurately and efficiently online, ensuring that you provide all necessary information to facilitate your claim.
Follow the steps to complete the form online with ease:
- Click ‘Get Form’ button to obtain the form and open it in your preferred editor.
- Begin filling out the form by entering the name of the beneficiary exactly as it appears on their health insurance card. Provide their last name, first name, and middle name in the respective fields.
- Enter the claim number from the health insurance card in the designated field.
- Indicate the patient's sex by selecting the appropriate option: male or female.
- Provide the patient's complete mailing address. Make sure to include the street address, including any apartment number, city, state, and zip code.
- Enter the patient's telephone number, including the area code. If the patient has moved recently, check the box indicating a new address.
- Describe the illness or injury for which the patient received treatment in a clear manner. Specify if the condition was related to the patient’s employment or an accident by checking the corresponding boxes.
- Answer the question about whether the patient has been treated with chronic dialysis or kidney transplant by checking 'Yes' or 'No'.
- If applicable, provide details regarding other health insurance coverage. Answer the questions about employment status and coverage under an employee health plan.
- Complete the section for other medical coverage by providing the name and address of the respective insurance or State Agency (Medicaid) and the policy number.
- Sign the form in the designated signature area, ensuring to include the date of signing. If the patient is unable to sign, refer to the instructions for Block 6 on the reverse.
- Lastly, remember to attach itemized bills from the doctors or suppliers to the back of this form before submission.
Complete your HHS CMS-1490 (Formerly CMS-1490S) online today to ensure timely processing of your medical payment claims.
Get form
Experience a faster way to fill out and sign forms on the web. Access the most extensive library of templates available.
Is CMS the same as Medicare? No. The Centers for Medicare & Medicaid Services (CMS) is part of the U.S. Department of Health and Human Services (HHS) and is not the same as Medicare. Medicare is a federally run government health insurance program, which is administered by CMS.
Get This Form Now!
Use professional pre-built templates to fill in and sign documents online faster. Get access to thousands of forms.