Loading
Get Va Chkd Authorization To Use Or Disclose Protected Health Information 2023-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the VA CHKD Authorization To Use Or Disclose Protected Health Information online
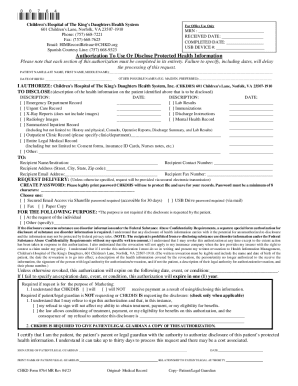
The VA CHKD Authorization To Use Or Disclose Protected Health Information form is an essential document that allows users to provide consent for the disclosure of their protected health information. This guide will walk you through the necessary steps to complete this form online.
Follow the steps to fill out the authorization form accurately.
- Press the ‘Get Form’ button to access the form and open it in your browser.
- Complete the patient name section by entering the last name, first name, and middle name of the individual whose information is being disclosed.
- Input the patient's date of birth in the designated field.
- If applicable, provide any other possible names of the patient, such as maiden or preferred names.
- Authorize Children's Hospital of The King's Daughters Health System, Inc. by ensuring the pre-filled name is correctly displayed.
- In the section for health information to be disclosed, select the relevant boxes that describe the health information. Be sure to specify additional details if needed.
- Enter the date associated with the disclosures you have selected.
- Fill in the recipient's information, including their name, contact number, address, email, and fax number as necessary.
- Choose the delivery method for the information — such as secured email, fax, or paper copy — depending on your preference.
- Provide a password for secured electronic transmission if you selected that option, ensuring it meets the minimum requirements.
- If required, select the purpose for the disclosure and provide any necessary additional explanation.
- Review the statements regarding revocation and expiration of the authorization, ensuring understanding before signing.
- Sign the form, print your name, and indicate your relationship to the patient, if applicable.
- Once completed, save your changes, and download, print, or share the form as required.
Complete your authorization forms online to ensure timely processing of your requests.
To receive your child's medical records, you must complete and send in the authorization form (PDF). A form is not complete unless a parent or guardian's written signature is on the form. You may fax the completed form to (414) 266-6316 or email it as an attachment to MedicalRecords@childrenswi.org.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.