Loading
Get Tx Flextra Dependent Care Reimbursement Claim Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the TX FLEXTRA Dependent Care Reimbursement Claim Form online
Filling out the TX FLEXTRA Dependent Care Reimbursement Claim Form online can streamline your reimbursement process for dependent care expenses. This guide provides clear, step-by-step instructions to help you navigate the form efficiently.
Follow the steps to complete your claim form seamlessly.
- Click ‘Get Form’ button to obtain the TX FLEXTRA Dependent Care Reimbursement Claim Form and access it in your preferred online format.
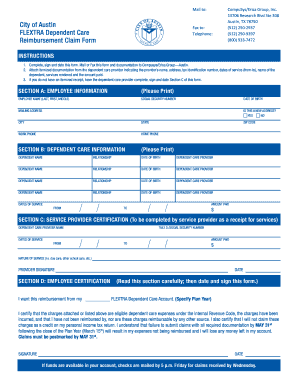
- Section A: Employee Information. Fill out your details, including your full name, social security number, date of birth, and mailing address. Indicate if this is a new address by selecting 'Yes' or 'No.' Input your city, state, work phone, and home phone.
- Section B: Dependent Care Information. Enter the name, relationship, and date of birth for each dependent. Include the dependent care provider's name for each entry. Continue this process for the number of dependents you are claiming.
- Provide the dates of service. Clearly document the range of dates for care provided, the ZIP code of the provider, and the total amount paid for services.
- Section C: Service Provider Certification. If required, ensure the dependent care provider fills out this section with their name, tax identification number, dates of service, nature of service, and total amount paid. Obtain their signature and the date.
- Section D: Employee Certification. Carefully read this section. Specify the plan year for reimbursement. Sign and date the form, affirming that all information and charges are accurate. Understand that claims must be submitted by May 31st following the close of the plan year.
- After completing all sections, review your inputs for accuracy. Save your changes, and then download, print, or share the form as necessary to submit your claim.
Begin your online submission process now to ensure your dependent care expenses are reimbursed.
To submit a reimbursement for your dependent care FSA, fill out the TX FLEXTRA Dependent Care Reimbursement Claim Form completely. Attach all necessary receipts and documentation required for your claim. Once your form is complete, send it to the designated address provided by your plan administrator. Keeping a copy of your submission is smart, just in case you need to reference it later.