Loading
Get Concentra Access And Authorization For Disclosure Of Protected Health Information (phi) Hipaa 2015-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Concentra Access And Authorization For Disclosure Of Protected Health Information (PHI) HIPAA online
Filling out the Concentra Access And Authorization For Disclosure Of Protected Health Information (PHI) HIPAA form is essential for managing your health information. This guide will provide you with step-by-step instructions to ensure you understand each section of the form as you complete it online.
Follow the steps to successfully complete your authorization form.
- Click the ‘Get Form’ button to access the authorization form and open it for use.
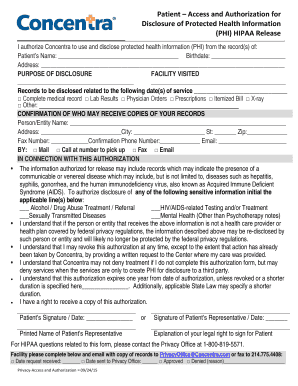
- Enter the patient's name in the designated field along with their birthdate and address. This information is required to identify the individual whose PHI is being disclosed.
- Indicate the purpose of the disclosure by specifying the facility visited. Write down the name or other identifying details of the facility in the provided space.
- Specify the records to be disclosed by checking the boxes next to the relevant items such as complete medical records, lab results, or other pertinent documents. Also include the related dates of service.
- Provide the name and address of the person or entity that may receive the copies of the records. Complete the necessary fields such as city, state, zip code, fax number, confirmation phone number, and email.
- Choose how the information will be shared by selecting one of the options: mail, call for pickup, fax, or email.
- If applicable, indicate any sensitive information that requires additional authorization by initializing the corresponding lines.
- Review the acknowledgment statements about the privacy regulations and rights concerning the authorization. Ensure you understand the implications of your choices.
- Sign and date the form at the designated areas. If applicable, include the printed name and explanation of the legal right to sign on behalf of the patient.
- Finally, save your changes, download a copy for your records, and share or print the completed authorization form as needed.
Complete your documents online today to ensure your health information is managed smoothly and securely.
I hereby authorize use or disclosure of protected health information about me as described below. I understand that the information used or disclosed may be subject to re-disclosure by the person or class of persons or facility receiving it, and would then no longer be protected by federal privacy regulations.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.