Loading
Get Oh Medicaid Managed Care Pharmacy Prior Authorization Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the OH Medicaid Managed Care Pharmacy Prior Authorization Request Form online
The OH Medicaid Managed Care Pharmacy Prior Authorization Request Form is essential for obtaining necessary medications. This guide provides step-by-step instructions to help users accurately complete and submit the form online.
Follow the steps to successfully complete your prior authorization request.
- Press the ‘Get Form’ button to access the OH Medicaid Managed Care Pharmacy Prior Authorization Request Form and open it in your preferred online editor.
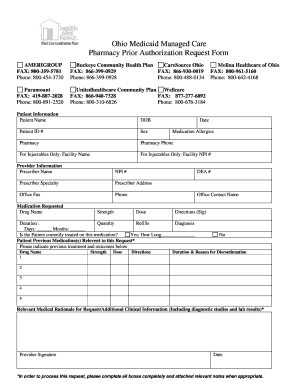
- Begin by filling out the patient information section. Provide the patient’s name, date of birth (DOB), patient ID number, and sex. Additionally, include the date of the request, pharmacy details, and the pharmacy's phone number. If the request is for injectables, also input the facility name and its National Provider Identifier (NPI) number.
- Next, move to the provider information section. Enter the prescriber’s name, medication allergies, NPI number, Drug Enforcement Administration (DEA) number, prescriber specialty, and their contact address. Make sure to include the provider's office fax number and phone number.
- In the medication requested section, fill out the drug name, strength, dosing requirements, and duration. Be sure to specify the quantity and number of refills needed. You will also need to indicate if the patient is currently being treated with this medication and detail how long they have been on it.
- List any previous medications relevant to this request, including the drug name, strength, dose, directions, and reasons for discontinuation if applicable. Provide details for up to five previous medications.
- Provide relevant medical rationale for the medication request, including any additional clinical information, diagnostic studies, or lab results that support the request.
- Finally, the prescriber must sign and date the form. Ensure all fields are completed accurately, and attach any relevant notes to support your request.
- Once you have completed and reviewed the form, you can save changes, download it, print it out, or share it as needed.
Complete your prior authorization request form online today for efficient processing.
As of October 1, Ohio Department of Medicaid's (ODM) Single Pharmacy Benefit Manager (SPBM), Gainwell Technologies, is responsible for managing pharmacy services including a specialty pharmacy program for all Medicaid managed care members.