Loading
Get Nasscorp Liberia Forms
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Nasscorp Liberia Forms online
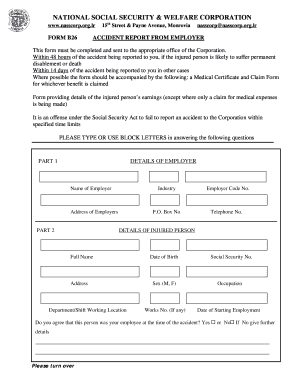
This guide provides a comprehensive overview of how to complete the Nasscorp Liberia Forms online, specifically focused on the Accident Report from Employer. By following these steps, users can ensure they fill out the form accurately and efficiently.
Follow the steps to complete the form successfully.
- Click ‘Get Form’ button to access the form and open it for editing.
- Begin with Part 1, which requires you to enter the details of the employer. Fill in the name of the employer, the industry, the P.O. Box number, and the address of the employer.
- In Part 2, provide the Employer Code Number and telephone number. Then, move to the details of the injured person by entering their full name, address, department or shift working location, date of birth, social security number, sex, occupation, works number (if applicable), and the date they started employment.
- Still in Part 2, indicate whether you agree that this person was your employee at the time of the accident by selecting 'Yes' or 'No.' If 'No,' please provide further details.
- In Part 3, fill out the details of the accident. Start with the date and time of the accident, as well as the location.
- Describe exactly what the injured person was doing at the time of the accident and indicate if it was an authorized task related to their job.
- If the accident occurred off your premises, explain why the injured person was at that location.
- Specify the hours the injured person was supposed to work on the day of the accident, their start time, and finish time.
- Describe how the accident happened briefly, and provide the names and addresses of at least two witnesses, if possible.
- Indicate when the accident was reported to you, the nature and extent of the injury, whether the injured person has returned to work, and details about their treatment.
- Lastly, confirm if you are paying wages to the injured person while they are absent from work. Select the applicable benefits you wish to claim, and ensure that you sign and date the form, entering your position and employer's stamp.
- Once you have completed all sections of the form, review the information for accuracy. Save your changes, and then download, print, or share the completed form as needed.
Complete your Nasscorp Liberia Forms online today for efficient processing of your accident report.
Old-Age Benefits Old-age pension (Retirement Pension): 25% of the insured's average monthly earnings plus 1% of average monthly earnings for every 10 months of contributions exceeding 144 months (100 months if born before 1980) is paid.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.