Loading
Get Wellcare Attestation Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Wellcare Attestation Form online
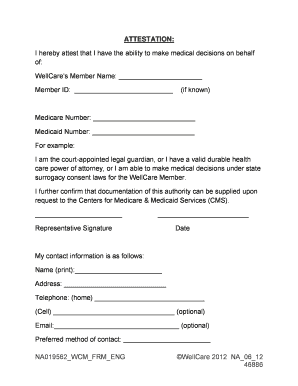
Filling out the Wellcare Attestation Form online is an essential step for individuals who need to confirm their authority to make medical decisions on behalf of a Wellcare member. This guide provides clear, step-by-step instructions to ensure the process is straightforward and user-friendly.
Follow the steps to successfully complete the form.
- Click the ‘Get Form’ button to access the Wellcare Attestation Form. This will open the form in a suitable editor for you to fill out.
- Begin by entering the Wellcare member's name and their member ID in the designated fields. If known, you should also include the Medicare Number and Medicaid Number.
- In the section that states your relationship to the member, clearly indicate your authority to make medical decisions by specifying if you are a court-appointed guardian or have a valid durable health care power of attorney.
- Provide a signature as the representative alongside the date to validate the attestation. Ensure that these entries are made in the designated areas.
- Fill out your contact information in the respective fields, including your name, address, and telephone numbers. Email and preferred methods of contact can be added optionally.
- Indicate where you wish for plan correspondence to be sent by checking the appropriate box, either to your address or the Wellcare member’s address.
- Designate witnesses by providing their names and the respective dates. Remember that these witnesses should not be associated with the representative, Wellcare member, or a healthcare facility.
- Once all sections are completed, ensure to review the information for accuracy. After confirming everything is correct, you can opt to save changes, download, print, or share the form.
Complete the Wellcare Attestation Form online today to ensure the necessary documentation is in place.
Visit ssbci.rrd.com. Follow the steps on ssbci.rrd.com to evaluate your patient against the eligibility requirements outlined on ssbci.rrd.com. Submit an attestation form through ssbci.rrd.com indicating your patient meets the eligibility requirements.