Get Mvp Health Care Claim Adjustment Request Form 2013-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MVP Health Care Claim Adjustment Request Form online
This guide provides step-by-step instructions for users looking to complete the MVP Health Care Claim Adjustment Request Form online. By following these clear directions, you can ensure that your adjustment request is submitted accurately and efficiently.
Follow the steps to complete the claim adjustment request form online.
- Click ‘Get Form’ button to obtain the Claim Adjustment Request Form and open it in the online editor.
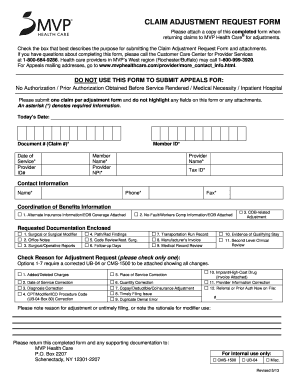
- Begin by entering today’s date in the designated field at the top of the form. This information helps track the timing of your submission.
- Fill out the Document # (Claim #)* field with the relevant claim number associated with the adjustment. This is an essential piece of information.
- Provide the Member ID* by entering the identification number for the member related to the claim. This helps to link the claim to the correct individual.
- Complete the Date of Service* field by stating the exact date when the service was provided. Accuracy here is crucial for the adjustment request.
- Enter the Provider ID# followed by the Provider NPI* in their respective fields. These identifiers are necessary to process the request correctly.
- Fill in the Provider Name* and Tax ID* fields to ensure the request is associated with the correct healthcare provider.
- Complete the Contact Information section by including your Name* and Phone* number, so that MVP can easily reach you if any questions arise.
- Select the appropriate box under the Coordination of Benefits Information section, ensuring you include any relevant alternate insurance information or documentation as indicated.
- Check the Reason for Adjustment Request section and select only one option that accurately describes why you are submitting this form.
- In the provided field, note the reason for adjustment or any necessary details regarding untimely filing or modifier use.
- Finally, review your completed form for accuracy. Once everything is correct, you can save your changes, download the form, or print it for submission. Make sure to attach any supporting documentation that is required.
Submit your Claim Adjustment Request Form online today to ensure timely processing of your claims.
Related links form
MVP Healthcare is not part of Cigna; they operate independently within the healthcare market. Both organizations provide health insurance, but they are separate companies with unique offerings. If you are looking for specific information related to MVP policies, the MVP Health Care Claim Adjustment Request Form is the recommended way to handle any adjustments or claims. Make sure to familiarize yourself with MVP’s specific processes.
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.