Loading
Get Ca Form 10133.36 2014-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CA Form 10133.36 online
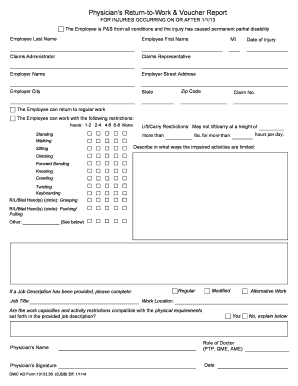
Filling out the CA Form 10133.36 accurately is essential for processing a return-to-work report related to permanent partial disability claims. This guide will take you through each section of the form step-by-step, ensuring you understand how to complete it efficiently online.
Follow the steps to successfully complete the form online.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
- Begin by entering the employee's last name and first name in the designated fields. This ensures that the report is linked correctly to the individual in question.
- Next, fill in the claims administrator's information along with the claims representative, ensuring to include their contact details for any follow-up.
- Enter the employer's name, street address, city, state, and zip code. Double-check these details for accuracy as they are essential for proper communication.
- Record the date of injury and claim number in their respective fields. This information is crucial for identifying the specific claim context.
- Indicate whether the employee can return to their regular work or if they require modified work with restrictions. Specify the number of hours they can stand, walk, or sit.
- Detail the lift/carry restrictions by stating the maximum height and weight the employee can handle. This should reflect the real-world limitations due to the injury.
- Provide descriptions of any limited activities such as climbing, bending, or keyboarding. For hand restrictions, specify which hand is affected.
- If applicable, complete the job description section if a job description has been provided. Confirm whether the employee’s capacities and restrictions align with the physical demands of the job.
- Conclude the form by entering the physician's name, their role, signing the document, and including the date of completion.
- Finally, review the entire form for accuracy, then save changes. You can download a copy for your records, print it, or share it as needed.
Complete your CA Form 10133.36 online today to ensure efficient processing of your return-to-work report.
The Division of Workers' Compensation (DWC) monitors the administration of workers' compensation claims, and provides administrative and judicial services to assist in resolving disputes that arise in connection with claims for workers' compensation benefits.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.