Loading
Get Wa F262-024-000 2017-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WA F262-024-000 online
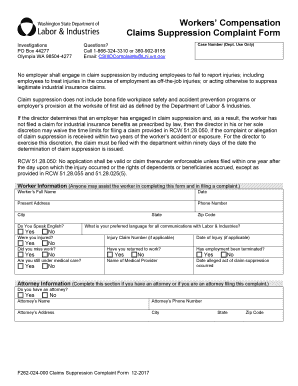
The WA F262-024-000 is the Claims Suppression Complaint Form designed to report any employer actions that may suppress legitimate workers’ compensation claims. This guide will provide step-by-step instructions to assist you in accurately completing this form online.
Follow the steps to successfully complete your complaint form.
- Press the ‘Get Form’ button to access the form and open it in your editor.
- Begin by entering the worker's full name in the designated field.
- Provide the date of completion in the appropriate section.
- Fill in the present address, including city, state, and zip code.
- Include the worker's phone number, ensuring it is accurate.
- Indicate whether the worker speaks English by selecting 'Yes' or 'No'.
- Specify the preferred language for all communications with Labor & Industries.
- Answer the question regarding injury status by selecting 'Yes' or 'No' and provide the injury claim number if applicable.
- Indicate the date of injury, if known.
- Answer the questions regarding missed work, return to work status, employment termination, and ongoing medical care.
- If applicable, provide the name of the medical provider.
- Enter the date when the alleged act of claim suppression occurred.
- Complete the attorney information section if applicable, including their name, phone number, and address.
- Provide detailed information about the employer including business name, type of business, phone number, and supervisor's name.
- Enter the date hired, department worked, job title, and full business address.
- Describe what the employer said or did to suppress the claim. Attach additional pages if necessary.
- List any witnesses to the employer’s actions, providing their names, addresses, and phone numbers.
- Indicate whether you have filed a complaint with any other agency and specify which one.
- Certify the accuracy of the information provided by printing the name, signing, and dating the form.
- Once all fields are completed, save your changes, and you can choose to download, print, or share the form.
Complete your complaint form online to ensure your rights are protected.
If you are injured at work, or have a work-related illness: Immediately report any work-related injury to your supervisor. If you require emergency medical treatment, obtain care first, and then notify your supervisor as soon as possible after receiving treatment.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.