Loading
Get Ca Ortho La Verification Of Work-related Injury 2020-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the CA Ortho LA Verification Of Work-Related Injury online
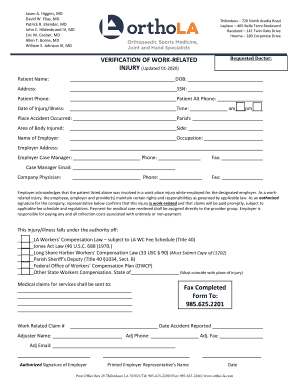
The CA Ortho LA Verification Of Work-Related Injury form is essential for documenting work-related injuries for patients. This guide provides a clear and supportive approach to help users fill out the form online with ease.
Follow the steps to fill out the CA Ortho LA Verification Of Work-Related Injury form online.
- Press the ‘Get Form’ button to access the Verification Of Work-Related Injury form. This will open the document in an online editor for your convenience.
- Begin by entering the patient’s name in the designated field. This must be the full legal name of the individual who sustained the injury.
- In the next section, input the patient's date of birth (DOB) in the appropriate format. This helps verify the identity of the patient.
- Provide the patient's address, ensuring all details such as street address and city are included.
- Enter the patient’s social security number (SSN) in the specified field. Be mindful to keep this information confidential.
- Fill in the patient’s phone number for any necessary follow-up communication regarding the injury.
- Document the date and time of the injury or illness, choosing either am or pm as appropriate.
- Indicate any alternative phone number for the patient, if available, to ensure they can be reached.
- Specify the place where the accident occurred, providing complete and accurate details.
- Select the parish where the injury took place, if applicable.
- Identify the area of the body that was injured and specify which side of the body is affected—left or right.
- Input the name of the employer and provide their address in the fields provided.
- Fill in the occupation of the patient to provide context about their role at the employer's establishment.
- Include the case manager's name, along with their phone number and fax number for communication purposes.
- Add the case manager’s email address, if available, to facilitate further correspondence.
- Identify the company physician’s name and contact details for additional medical support.
- Confirm that the employer acknowledges the work-related injury and understand their responsibilities regarding compensation.
- Select the relevant authority under which the injury falls, marking the appropriate boxes as necessary.
- Provide the medical claims address, ensuring all relevant details are included for where the claims should be sent.
- Fill out the work-related claim number if applicable, ensuring it corresponds with the specific case.
- Complete the section for faxing the completed form, mainly, the number 985.625.2201.
- Enter the date when the accident was reported to ensure an accurate timeline.
- Add the adjuster’s name, phone number, fax number, and email for clarity in claims handling.
- The authorized employer representative should sign and print their name along with the date of signing.
- Once all information is complete, save your changes. You can download, print, or share the form as needed.
Complete your CA Ortho LA Verification Of Work-Related Injury form online today to ensure timely processing of your claims.
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.