Loading
Get Wa Chpw Mental Health Service Prior Authorization Request Form 2020-2025
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the WA CHPW Mental Health Service Prior Authorization Request Form online
Filling out the WA CHPW Mental Health Service Prior Authorization Request Form online can streamline the process for obtaining necessary mental health services. This guide will help you navigate each section of the form with clarity and ease.
Follow the steps to complete the form accurately and efficiently.
- Click ‘Get Form’ button to access the form and open it in your online editor.
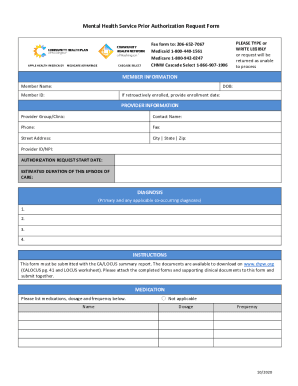
- Begin by entering member information in the designated fields. This includes the member's full name, date of birth, and member ID. If applicable, provide the retroactive enrollment date.
- Next, fill in the provider information section. Enter the provider group or clinic name, the contact person’s name, and all necessary contact information including phone and fax numbers, street address, city, state, and zip code, as well as the provider ID or NPI.
- Specify the authorization request start date and the estimated duration of the care episode.
- List all relevant diagnoses in the Diagnosis section. You can include up to four primary and co-occurring diagnoses.
- Ensure you have the CA/LOCUS summary report ready to submit with the form as instructed. This is required documentation.
- In the medication section, provide the medication names, including dosage and frequency. If no medications are applicable, check the corresponding box.
- Indicate the CA/LOCUS level of care based on the score. Choose from options listed such as Level 3, Level 4, Level 5, or Level 6.
- Complete the section on the requested level of care, indicating if it differs from the CA/LOCUS recommendation. If it does vary, provide a clear reason and attach supporting clinical documentation.
- Fill in the requested codes and specify the units or visits needed for each code. Be sure to include any applicable modifiers for the requested services.
- Finally, review all information for accuracy. Have the reviewer print their name, sign, and date the form.
- Once you have completed the form, make sure to save the changes. You may also download, print, or share the document as needed.
Start completing your WA CHPW Mental Health Service Prior Authorization Request Form online today!
Industry-leading security and compliance
US Legal Forms protects your data by complying with industry-specific security standards.
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.