Loading
Get Priority Partners Pharmacy Prior Authorization Form 2014-2026
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Priority Partners Pharmacy Prior Authorization Form online
Filling out the Priority Partners Pharmacy Prior Authorization Form accurately is essential to ensure timely processing of your prior authorization request. This guide will provide clear, step-by-step instructions to help you complete the form efficiently online.
Follow the steps to complete the form online.
- Click ‘Get Form’ button to obtain the form and access it for completion.
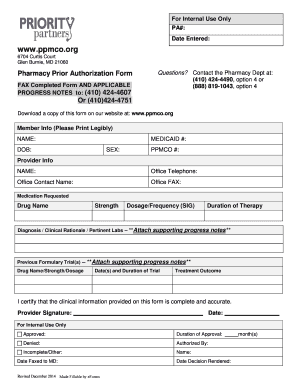
- Begin by filling out the Member Info section. Ensure to include the member's name, Medicaid number, date of birth, and PPMCO number. Please print legibly to avoid any processing delays.
- In the Provider Info section, enter the provider's name, office telephone number, office contact name, and office fax number. Providing accurate contact details is vital for any follow-ups.
- Next, enter the Medication Requested details. Fill in the drug name, strength, and dosage/frequency (SIG) of the requested medication.
- For the Diagnosis / Clinical Rationale / Pertinent Labs section, briefly describe the clinical rationale for the medication and any pertinent lab results. **Remember to attach supporting progress notes.**
- Detail any previous formulary trials, including the drug name, strength, dosage, dates, duration of the trial, and treatment outcomes. This information helps support your request.
- You or an authorized provider must certify the accuracy of the information by signing the form and entering the date of the signature.
- Review the completed form carefully to ensure all required information is accurate and legible. Then, you can save the changes, download a copy, print the form, or share it as necessary.
Ensure you complete the Priority Partners Pharmacy Prior Authorization Form online today to facilitate your request.
Related links form
For additional information on EDI (Electronic Data Interchange), please send an email request to edi@jhhc.com. EDI Payor ID #58379.