Get Mvp Health Care Claim Adjustment Request Form 2010
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the MVP Health Care Claim Adjustment Request Form online
Filling out the MVP Health Care Claim Adjustment Request Form online can be a straightforward process if followed correctly. This guide provides clear step-by-step instructions to help you complete the form accurately and efficiently.
Follow the steps to successfully complete your claim adjustment request.
- Click ‘Get Form’ button to access the form and open it in your preferred editor.
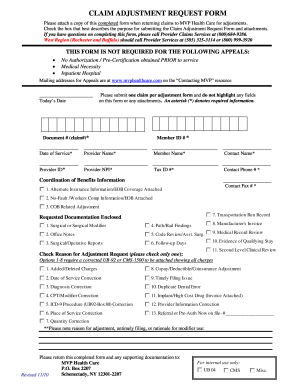
- Enter today's date in the designated field at the top of the form.
- Complete the required fields for the document number (claim #), member ID#, and date of service. These fields are marked with an asterisk (*) and must be filled in for processing.
- Fill in the provider name, member name, contact name, provider ID, NPI, tax ID, and contact phone number. Ensure that all information is accurate and up-to-date.
- Provide coordination of benefits information, including alternate insurance details, and if applicable, include any additional required documentation by checking the relevant boxes.
- Select a reason for the adjustment request by checking only one of the provided options. Ensure an appropriate corrected UB-92 or CMS-1500 is attached when necessary.
- Provide a brief explanation for the reason behind the adjustment request, addressing any additional notes regarding filing issues or modifiers.
- Review the completed form for any errors or omissions to ensure accuracy.
- Once all fields are filled out, save your changes. You can download, print, or share the form as needed.
Complete your MVP Health Care Claim Adjustment Request Form online today and ensure your claims are processed efficiently.
Get form
Related links form
US Legal Forms offers a comprehensive library of legal documents, including the MVP Health Care Claim Adjustment Request Form. You can easily find and download forms tailored to your needs, streamlining the claim adjustment process. Additionally, they provide guidance on how to fill out these forms correctly. This can save you time and reduce the stress involved in managing healthcare claims.
Get This Form Now!
Industry-leading security and compliance
-
In businnes since 199725+ years providing professional legal documents.
-
Accredited businessGuarantees that a business meets BBB accreditation standards in the US and Canada.
-
Secured by BraintreeValidated Level 1 PCI DSS compliant payment gateway that accepts most major credit and debit card brands from across the globe.