Loading
Get Cdn.cocodoc.comcocodoc-form-pdfpdfsleep Study Prior Authorization Request Form
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the Cdn.cocodoc.comcocodoc-form-pdfpdfSleep Study Prior Authorization Request Form online
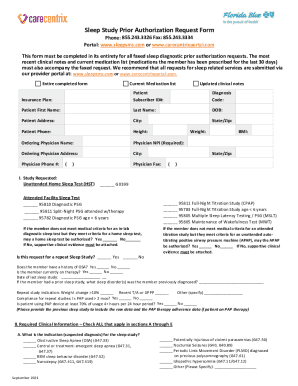
The Sleep Study Prior Authorization Request Form is essential for obtaining approval for sleep diagnostic testing. This guide will assist users in accurately completing the form online, ensuring all necessary information is provided to facilitate a smooth authorization process.
Follow the steps to fill out the Sleep Study Prior Authorization Request Form online.
- Press the ‘Get Form’ button to access and open the Sleep Study Prior Authorization Request Form.
- Fill in the 'Patient' section with the patient's first and last name, date of birth, address (including city, state, and zip code), and phone number. Ensure all personal details are accurate.
- Provide 'Insurance Plan' information along with the 'Subscriber ID#', ensuring these details match the patient’s insurance documentation.
- Enter the diagnosis code relevant to the patient's condition, ensuring that the correct code is used. This is crucial for authorization approval.
- In the 'Ordering Physician' section, fill in the physician's name, NPI number, address, phone number, and fax number. The physician's NPI is a required field, so confirm its accuracy.
- Indicate the type of study requested by checking the appropriate box (e.g., Unattended Home Sleep Test, Attended Facility Sleep Test, etc.).
- Respond to the questions regarding medical criteria for sleep tests by checking 'Yes' or 'No', as applicable. Attach supportive clinical evidence if required.
- In the 'Required Clinical Information' section, check all relevant indications, signs, symptoms, and comorbid conditions that apply to the patient. This information helps justify the prior authorization request.
- Specify the billing sleep test provider's name, address, phone number, fax number, tax ID, and NPI, if applicable. This information helps coordinate billing and services.
- For Florida Blue sleep diagnostic requests, select and circle the place of service from the provided options, as this is a required field.
- In the 'Special Needs' section, include any information on cognitive impairments or language needs pertinent to the patient's situation.
- Verify the accuracy of the provided information by checking the verification box. Sign with the verifying person's name and date the form appropriately.
- Save any changes made, then proceed to download, print, or share the completed form based on your needs.
Complete your Sleep Study Prior Authorization Request Form online today for efficient processing.
Provider Central For:Fax: Blue Cross Blue Shield of Massachusetts Employees BCBSMA employees: authorizations, referrals and InterQual Smart Sheets TM Surgical forms 617-246-4299 BCBSMA employees: behavioral health/substance use authorizations and neuropsychological testing 1-888-608-369316 more rows