Loading
Get Dss-2949
How it works
-

Open form follow the instructions
-

Easily sign the form with your finger
-

Send filled & signed form or save
How to fill out the DSS-2949 online
Filling out the DSS-2949 is an essential step in documenting personal and health information for residents. This guide provides you with clear, step-by-step instructions to complete the form online effectively.
Follow the steps to complete the DSS-2949 without hassle.
- Click ‘Get Form’ button to obtain the form and open it in the editor.
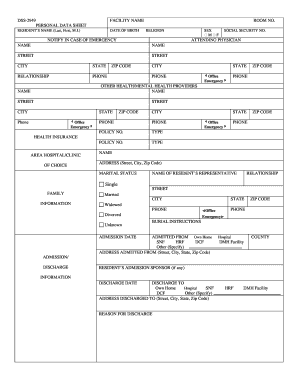
- Begin by entering the facility name and room number where applicable, ensuring accurate information as this identifies the location of the resident.
- Fill out the personal data section, including the resident's name (last, first, M.I.), date of birth, and religion. Be attentive to each field to ensure correctness.
- In the ‘Notify in case of emergency’ section, provide the name, address, relationship, and phone number of a designated contact who can be reached in an emergency.
- Enter the social security number, attending physician’s name, and their contact information, including city, state, and phone number.
- List any other health or mental health providers by filling in their names, addresses, and phone numbers in the respective fields.
- Indicate the health insurance information by specifying the policy number and type, ensuring that the details are accurate and up to date.
- Select the area hospital or clinic of choice, providing complete address details.
- Complete the marital status section accurately, identifying whether the resident is single, married, widowed, divorced, or if the status is unknown.
- In the burial instructions section, specify any relevant details as needed.
- Provide information on the admission date and from where the resident was admitted (options include own home, hospital, SNF, HRF, DCF, or other). Include the full address of the place admitted from.
- Fill out the discharge date and where the resident will be discharged to with similar options, ensuring all contact details are provided accurately.
- Conclude by reviewing the entire form for any inaccuracies or missing information and saving the changes, downloading, printing, or sharing the completed document as necessary.
Complete your DSS-2949 and other documents online today for streamlined processing.